Articles
- Page Path
- HOME > Acute Crit Care > Volume 34(2); 2019 > Article
-
Review Article
Rapid response system Rapid response systems in Korea -
Bo Young Lee1
 , Sang-Bum Hong2
, Sang-Bum Hong2 -
Acute and Critical Care 2019;34(2):108-116.
DOI: https://doi.org/10.4266/acc.2019.00535
Published online: May 31, 2019
1Division of Allergy and Respiratory Diseases, Department of Internal Medicine, Soonchunhyang University Hospital, Seoul, Korea
2Department of Pulmonary and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- Corresponding author Sang-Bum Hong Department of Pulmonary and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpa-gu, Seoul 05505, Korea Tel: +82-2-3010-3130 Fax: +82-2-3010-6968 E-mail: sbhong@amc.seoul.kr
Copyright © 2019 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
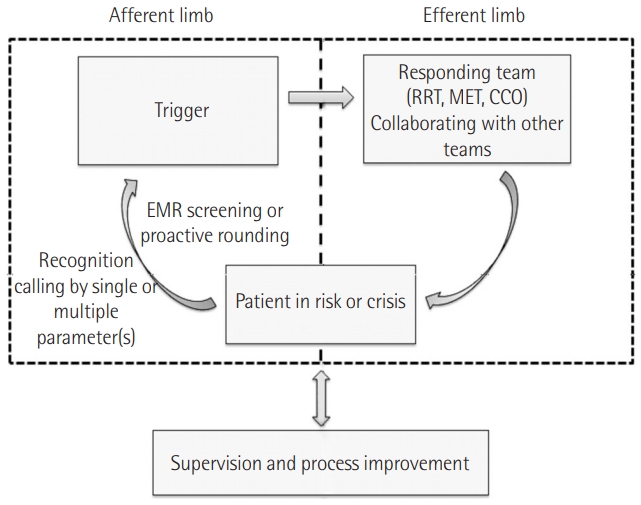
- The inpatient treatment process is becoming more and more complicated with advanced treatments, aging of the patient population, and multiple comorbidities. During the process, patients often experience unexpected deterioration, about half of which might be preventable. Early identification of patient deterioration and the proper response are priorities in most healthcare facilities. A rapid response system (RRS) is a safety net to identify antecedents of these adverse events and to respond in a timely manner. The RRS has become an essential part of the medical system worldwide, supported by all major quality improvement organizations. An RRS consists of a trigger system and response team and needs constant assessment and process improvement. Although the effectiveness and cost-benefit of RRS remain controversial, according to previous studies, it may be beneficial by decreasing in-hospital cardiac arrest and mortality. Since the first implementation of RRS in Korea in 2008, it has been developed in over 15 medical centers and continues to expand. Recent accreditation standards and an RRS pilot program by the Korean government will promote the proliferation of RRSs in Korea.
INTRODUCTION
RAPID RESPONSE SYSTEM
CONCLUSIONS
KEY MESSAGES
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conceptualization, Data curation, & Visualization: BYL, SBH. Writing-original draft: BYL. Writing-review & editing: SBH.
NOTES
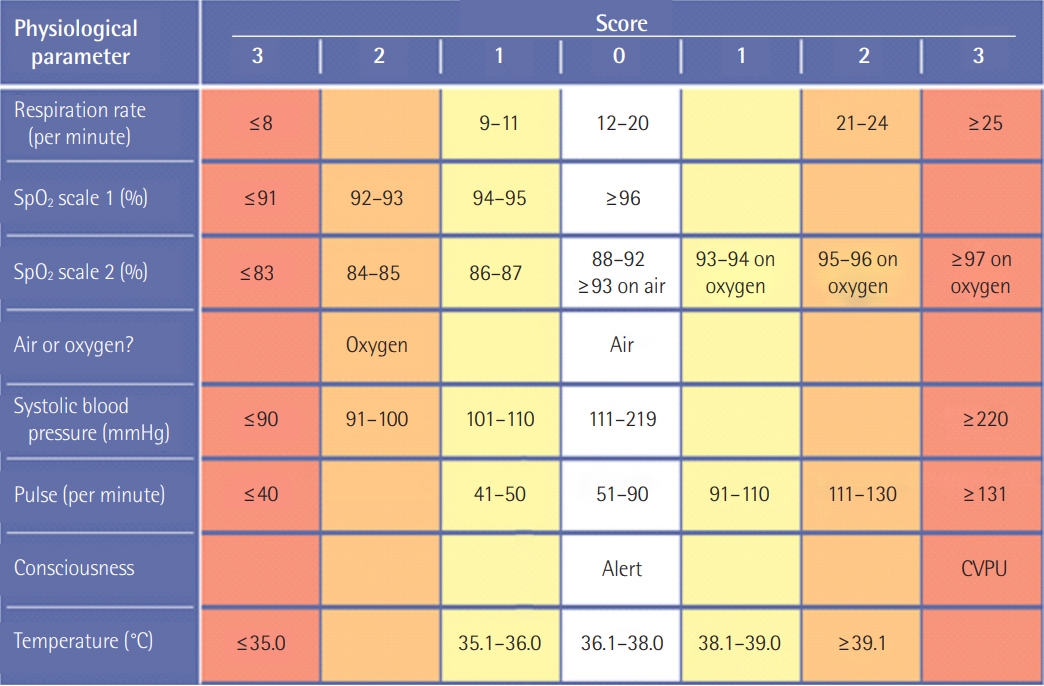
Reproduced from Subbe et al. QJM 2001;94:521-6, with permission of Oxford University Press [20].
AVPU: A, alert; V, responding to voice; P, responding to pain; U, unresponsive.
| Study |
Sample size |
Mortality rate per 1,000 admissions (%) |
OR of death (95% CI) | ||
|---|---|---|---|---|---|
| Control group | RRT group | Control group | RRT group | ||
| Observational and before-and-after study | |||||
| Buist et al. [31] | 19,317 | 22,847 | 19.7 | 17.2 | 0.87 (0.71–1.01) |
| Bellomo et al. [7] | 21,090 | 20,921 | 14.3 | 10.6 | 0.74 (0.70–0.79) |
| Bellomo et al. [32] | 1,116 | 1,067 | 65.4 | 42.2 | 0.64 (0.45–0.93) |
| Jones et al. [30] | 16,246 | 104,001 | 53.7 | 39.1 | 0.73 (0.68–0.78) |
| Chan et al. [27] | 24,193 | 24,978 | 32.2 | 30.9 | 0.95 (0.81–1.11) |
| Konrad et al. [26] | 203,892 | 73,825 | 18.9 | 16.4 | 0.90 (0.84–0.97) |
| Salvatierra et al. [11] | |||||
| Cluster-randomized study | 235,718 | 235,344 | 13.5 | 10.3 | 0.76 (0.72–0.80) |
| Priestley et al. [29] | 1,336 | 1,456 | 56.9 | 50.1 | 0.52 (0.32–0.85) |
| Hillman et al. [4] | 56,756 | 68,376 | 1.2 | 1.1 | 1.03 (0.84–1.28) |
- 1. Neale G, Woloshynowych M, Vincent C. Exploring the causes of adverse events in NHS hospital practice. J R Soc Med 2001;94:322-30.ArticlePubMedPMC
- 2. Jones DA, DeVita MA, Bellomo R. Rapid-response teams. N Engl J Med 2011;365:139-46.ArticlePubMed
- 3. Devita MA, Bellomo R, Hillman K, Kellum J, Rotondi A, Teres D, et al. Findings of the first consensus conference on medical emergency teams. Crit Care Med 2006;34:2463-78.ArticlePubMed
- 4. Hillman K, Chen J, Cretikos M, Bellomo R, Brown D, Doig G, et al. Introduction of the medical emergency team (MET) system: a cluster-randomised controlled trial. Lancet 2005;365:2091-7.ArticlePubMed
- 5. Chan PS, Jain R, Nallmothu BK, Berg RA, Sasson C. Rapid response teams: a systematic review and meta-analysis. Arch Intern Med 2010;170:18-26.ArticlePubMed
- 6. Jones D, Bellomo R, DeVita MA. Effectiveness of the Medical Emergency Team: the importance of dose. Crit Care 2009;13:313. ArticlePubMedPMC
- 7. Bellomo R, Goldsmith D, Uchino S, Buckmaster J, Hart GK, Opdam H, et al. A prospective before-and-after trial of a medical emergency team. Med J Aust 2003;179:283-7.ArticlePubMed
- 8. Sebat F, Musthafa AA, Johnson D, Kramer AA, Shoffner D, Eliason M, et al. Effect of a rapid response system for patients in shock on time to treatment and mortality during 5 years. Crit Care Med 2007;35:2568-75.ArticlePubMed
- 9. Buist M, Harrison J, Abaloz E, Van Dyke S. Six year audit of cardiac arrests and medical emergency team calls in an Australian outer metropolitan teaching hospital. BMJ 2007;335:1210-2.ArticlePubMedPMC
- 10. Jung B, Daurat A, De Jong A, Chanques G, Mahul M, Monnin M, et al. Rapid response team and hospital mortality in hospitalized patients. Intensive Care Med 2016;42:494-504.ArticlePubMedPDF
- 11. Salvatierra G, Bindler RC, Corbett C, Roll J, Daratha KB. Rapid response team implementation and in-hospital mortality. Crit Care Med 2014;42:2001-6.ArticlePubMed
- 12. Wilson RM, Runciman WB, Gibberd RW, Harrison BT, Newby L, Hamilton JD. The quality in Australian Health Care Study. Med J Aust 1995;163:458-71.ArticlePubMed
- 13. Schwendimann R, Blatter C, Dhaini S, Simon M, Ausserhofer D. The occurrence, types, consequences and preventability of in-hospital adverse events: a scoping review. BMC Health Serv Res 2018;18:521. ArticlePubMedPMCPDF
- 14. Schein RM, Hazday N, Pena M, Ruben BH, Sprung CL. Clinical antecedents to in-hospital cardiopulmonary arrest. Chest 1990;98:1388-92.ArticlePubMed
- 15. Buist M, Bernard S, Nguyen TV, Moore G, Anderson J. Association between clinically abnormal observations and subsequent in-hospital mortality: a prospective study. Resuscitation 2004;62:137-41.ArticlePubMed
- 16. Andersen LW, Kim WY, Chase M, Berg KM, Mortensen SJ, Moskowitz A, et al. The prevalence and significance of abnormal vital signs prior to in-hospital cardiac arrest. Resuscitation 2016;98:112-7.ArticlePubMed
- 17. Smith GB, Prytherch DR, Schmidt P, Featherstone PI, Knight D, Clements G, et al. Hospital-wide physiological surveillancea new approach to the early identification and management of the sick patient. Resuscitation 2006;71:19-28.ArticlePubMed
- 18. Levy MM, Evans LE, Rhodes A. The surviving sepsis campaign bundle: 2018 update. Crit Care Med 2018;46:997-1000.ArticlePubMed
- 19. Taenzer AH, Spence BC. The afferent limb of rapid response systems: continuous monitoring on general care units. Crit Care Clin 2018;34:189-98.ArticlePubMed
- 20. Subbe CP, Kruger M, Rutherford P, Gemmel L. Validation of a modified Early Warning Score in medical admissions. QJM 2001;94:521-6.ArticlePubMedPDF
- 21. McGaughey J, Alderdice F, Fowler R, Kapila A, Mayhew A, Moutray M. Outreach and Early Warning Systems (EWS) for the prevention of intensive care admission and death of critically ill adult patients on general hospital wards. Cochrane Database Syst Rev 2007;(3):CD005529. ArticlePubMed
- 22. Royal College of Physicians. National Early Warning Score (NEWS) 2: standardising the assessment of acute-illness severity in the NHS. London, Royal College of Physicians. 2017.
- 23. Berwick DM, Calkins DR, McCannon CJ, Hackbarth AD. The 100,000 lives campaign: setting a goal and a deadline for improving health care quality. JAMA 2006;295:324-7.ArticlePubMed
- 24. The Joint Commission announces the 2009 National Patient Safety Goals and requirements. Jt Comm Perspect 2008;28:111-5.
- 25. Kronick SL, Kurz MC, Lin S, Edelson DP, Berg RA, Billi JE, et al. Part 4: systems of care and continuous quality improvement. 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2015;132(18 Suppl 2):S397-413.ArticlePubMed
- 26. Konrad D, Jäderling G, Bell M, Granath F, Ekbom A, Martling CR. Reducing in-hospital cardiac arrests and hospital mortality by introducing a medical emergency team. Intensive Care Med 2010;36:100-6.ArticlePubMedPDF
- 27. Chan PS, Khalid A, Longmore LS, Berg RA, Kosiborod M, Spertus JA. Hospital-wide code rates and mortality before and after implementation of a rapid response team. JAMA 2008;300:2506-13.ArticlePubMed
- 28. Edelson DP, Yuen TC, Mancini ME, Davis DP, Hunt EA, Miller JA, et al. Hospital cardiac arrest resuscitation practice in the United States: a nationally representative survey. J Hosp Med 2014;9:353-7.ArticlePubMedPMC
- 29. Priestley G, Watson W, Rashidian A, Mozley C, Russell D, Wilson J, et al. Introducing Critical Care Outreach: a ward-randomised trial of phased introduction in a general hospital. Intensive Care Med 2004;30:1398-404.ArticlePubMedPDF
- 30. Jones D, Bellomo R, Bates S, Warrillow S, Goldsmith D, Hart G, et al. Long term effect of a medical emergency team on cardiac arrests in a teaching hospital. Crit Care 2005;9:R808-15.ArticlePubMedPMC
- 31. Buist MD, Moore GE, Bernard SA, Waxman BP, Anderson JN, Nguyen TV. Effects of a medical emergency team on reduction of incidence of and mortality from unexpected cardiac arrests in hospital: preliminary study. BMJ 2002;324:387-90.ArticlePubMedPMC
- 32. Bellomo R, Goldsmith D, Uchino S, Buckmaster J, Hart G, Opdam H, et al. Prospective controlled trial of effect of medical emergency team on postoperative morbidity and mortality rates. Crit Care Med 2004;32:916-21.ArticlePubMed
- 33. Maharaj R, Raffaele I, Wendon J. Rapid response systems: a systematic review and meta-analysis. Crit Care 2015;19:254. ArticlePubMedPMCPDF
- 34. ANZICS-CORE MET dose investigators. Mortality of rapid response team patients in Australia: a multicentre study. Crit Care Resusc 2013;15:273-8.ArticlePubMed
- 35. Huh JW, Lim CM, Koh Y, Lee J, Jung YK, Seo HS, et al. Activation of a medical emergency team using an electronic medical recording-based screening system. Crit Care Med 2014;42:801-8.ArticlePubMed
- 36. Kwak HJ, Yun I, Kim SH, Sohn JW, Shin DH, Yoon HJ, et al. The extended rapid response system: 1-year experience in a university hospital. J Korean Med Sci 2014;29:423-30.ArticlePubMedPMC
- 37. Lee YJ, Park JJ, Yoon YE, Kim JW, Park JS, Kim T, et al. Successful implementation of a rapid response system in the department of internal medicine. Korean J Crit Care Med 2014;29:77-82.Article
- 38. Kim Y, Lee DS, Min H, Choi YY, Lee EY, Song I, et al. Effectiveness analysis of a part-time rapid response system during operation versus nonoperation. Crit Care Med 2017;45:e592-9.ArticlePubMed
- 39. Park Y, Ahn JJ, Kang BJ, Lee YS, Ha SO, Min JS, et al. Rapid response systems reduce in-hospital cardiopulmonary arrest: a pilot study and motivation for a nationwide survey. Korean J Crit Care Med 2017;32:231-9.ArticlePubMedPMCPDF
- 40. Song JU, Suh GY, Park HY, Lim SY, Han SG, Kang YR, et al. Early intervention on the outcomes in critically ill cancer patients admitted to intensive care units. Intensive Care Med 2012;38:1505-13.ArticlePubMedPDF
- 41. Lee SH, Leem AY, Nho Y, Kim YA, Kim KD, Kim YS, et al. A pilot study of the effectiveness of medical emergency system implementation at a single center in Korea. Korean J Crit Care Med 2017;32:133-41.ArticlePubMedPMCPDF
- 42. Kim SW, Lee HY, Han MR, Lee YS, Kang EH, Jang EJ, et al. Epidemiology and clinical characteristics of rapid response team activations. Korean J Crit Care Med 2017;32:124-32.ArticlePubMedPMCPDF
- 43. Lee DH, Han M, An JY, Jung JY, Koh Y, Lim CM, et al. Video laryngoscopy versus direct laryngoscopy for tracheal intubation during in-hospital cardiopulmonary resuscitation. Resuscitation 2015;89:195-9.ArticlePubMed
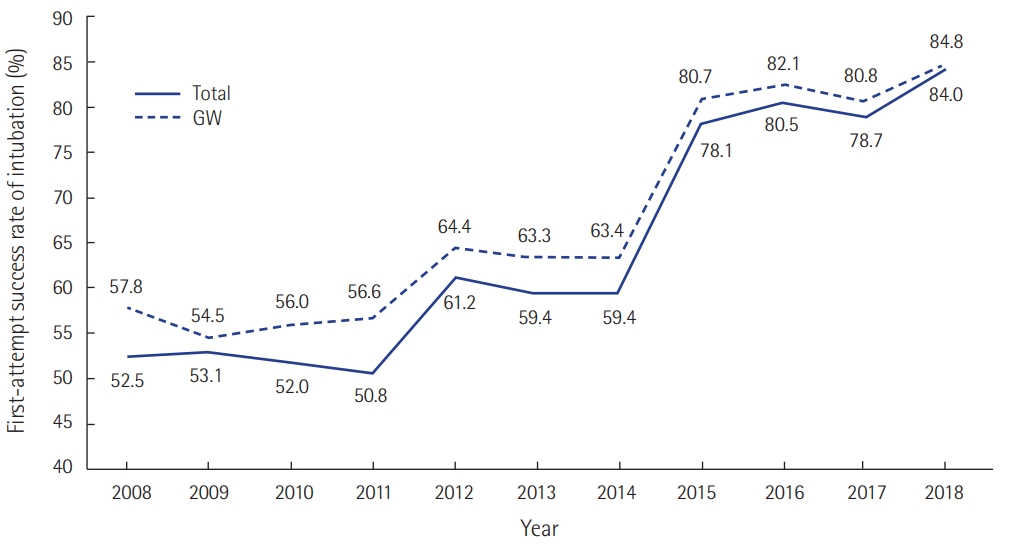
- 44. Baek MS, Han M, Huh JW, Lim CM, Koh Y, Hong SB. Video laryngoscopy versus direct laryngoscopy for first-attempt tracheal intubation in the general ward. Ann Intensive Care 2018;8:83. ArticlePubMedPMCPDF
- 45. Lyons PG, Edelson DP, Churpek MM. Rapid response systems. Resuscitation 2018;128:191-7.ArticlePubMedPMC
- 46. Lee Y, Kwon JM, Lee Y, Park H, Cho H, Park J. Deep learning in the medical domain: predicting cardiac arrest using deep learning. Acute Crit Care 2018;33:117-20.ArticlePubMedPMCPDF
References
Figure & Data
References
Citations
- Association between the timing of ICU admission and mortality in patients with hospital-onset sepsis: a nationwide prospective cohort study
Yoon Hae Ahn, Jinwoo Lee, Dong Kyu Oh, Su Yeon Lee, Mi Hyeon Park, Haein Lee, Chae-Man Lim, Sang-Min Lee, Hong Yeul Lee, Chae-Man Lim, Sang-Bum Hong, Dong Kyu Oh, Gee Young Suh, Kyeongman Jeon, Ryoung-Eun Ko, Young-Jae Cho, Yeon Joo Lee, Sung Yoon Lim, Su
Journal of Intensive Care.2023;[Epub] CrossRef - Findings from a decade of experience following implementation of a Rapid Response System into an Asian hospital
Augustine Tee, Bryan Peide Choo, Roshni Sadashiv Gokhale, Xiqin Wang, Mashithah Mansor, Hong Choon Oh, Daryl Jones
Resuscitation Plus.2023; 16: 100461. CrossRef - Development of a comprehensive model for the role of the rapid response team nurse
Youn-Hui Won, Jiyeon Kang
Intensive and Critical Care Nursing.2022; 68: 103136. CrossRef - Characteristics and outcomes of patients screened by rapid response team who transferred to the intensive care unit
Song-I. Lee, Jeong Suk Koh, Yoon Joo Kim, Da Hyun Kang, Jeong Eun Lee
BMC Emergency Medicine.2022;[Epub] CrossRef - Mortality of patients with hospital-onset sepsis in hospitals with all-day and non-all-day rapid response teams: a prospective nationwide multicenter cohort study
Dong-gon Hyun, Su Yeon Lee, Jee Hwan Ahn, Jin Won Huh, Sang-Bum Hong, Younsuck Koh, Chae-Man Lim, Dong Kyu Oh, Gee Young Suh, Kyeongman Jeon, Ryoung-Eun Ko, Young-Jae Cho, Yeon Joo Lee, Sung Yoon Lim, Sunghoon Park, Jeongwon Heo, Jae-myeong Lee, Kyung Cha
Critical Care.2022;[Epub] CrossRef - Korean nurses’ perception and performance on communication with physicians in clinical deterioration
Bo-Gyeong Jin, Kyoungrim Kang, Hyun-Jin Cho
Medicine.2022; 101(38): e30570. CrossRef - Clinical Nurses’ Intention to Use Defibrillators in South Korea: A Path Analysis
Dongchoon Uhm, Gye-Hyun Jung
Healthcare.2022; 11(1): 61. CrossRef - Rapid Response System Should Be Enhanced at Non-general Ward Locations: a Retrospective Multicenter Cohort Study in Korea
Byung Ju Kang, Sang-Bum Hong, Kyeongman Jeon, Sang-Min Lee, Dong Hyun Lee, Jae Young Moon, Yeon Joo Lee, Jung Soo Kim, Jisoo Park, Jong-Joon Ahn
Journal of Korean Medical Science.2021;[Epub] CrossRef - Impact of hospitalization duration before medical emergency team activation: A retrospective cohort study
Jinmi Lee, Yujung Shin, Eunjoo Choi, Sunhui Choi, Jeongsuk Son, Youn Kyung Jung, Sang-Bum Hong, Tai-Heng Chen
PLOS ONE.2021; 16(2): e0247066. CrossRef - A multicentre validation study of the deep learning-based early warning score for predicting in-hospital cardiac arrest in patients admitted to general wards
Yeon Joo Lee, Kyung-Jae Cho, Oyeon Kwon, Hyunho Park, Yeha Lee, Joon-Myoung Kwon, Jinsik Park, Jung Soo Kim, Man-Jong Lee, Ah Jin Kim, Ryoung-Eun Ko, Kyeongman Jeon, You Hwan Jo
Resuscitation.2021; 163: 78. CrossRef - Characteristics and Prognosis of Hospitalized Patients at High Risk of Deterioration Identified by the Rapid Response System: a Multicenter Cohort Study
Sang Hyuk Kim, Ji Young Hong, Youlim Kim
Journal of Korean Medical Science.2021;[Epub] CrossRef - Predicting severe outcomes using national early warning score (NEWS) in patients identified by a rapid response system: a retrospective cohort study
Sang Hyuk Kim, Hye Suk Choi, Eun Suk Jin, Hayoung Choi, Hyun Lee, Sang-Hwa Lee, Chang Youl Lee, Myung Goo Lee, Youlim Kim
Scientific Reports.2021;[Epub] CrossRef - A physician-led medical emergency team increases the rate of medical interventions: A multicenter study in Korea
Su Yeon Lee, Jee Hwan Ahn, Byung Ju Kang, Kyeongman Jeon, Sang-Min Lee, Dong Hyun Lee, Yeon Joo Lee, Jung Soo Kim, Jisoo Park, Jae Young Moon, Sang-Bum Hong, Amit Bahl
PLOS ONE.2021; 16(10): e0258221. CrossRef - Incorporating a real-time automatic alerting system based on electronic medical records could improve rapid response systems: a retrospective cohort study
Seung-Hun You, Sun-Young Jung, Hyun Joo Lee, Sulhee Kim, Eunjin Yang
Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine.2021;[Epub] CrossRef - Effects of a Rapid Response Team on the Clinical Outcomes of Cardiopulmonary Resuscitation of Patients Hospitalized in General Wards
Mi-Jung Yoon, Jin-Hee Park
Journal of Korean Academy of Fundamentals of Nursing.2021; 28(4): 491. CrossRef - Early Warning Score and Cancer Patients at End-of-Life
Jae-woo Lee, Ye-Seul Kim, Yonghwan Kim, Hyo-Sun Yoo, Hee-Taik Kang
Korean Journal of Clinical Geriatrics.2021; 22(2): 67. CrossRef - Effectiveness of a daytime rapid response system in hospitalized surgical ward patients
Eunjin Yang, Hannah Lee, Sang-Min Lee, Sulhee Kim, Ho Geol Ryu, Hyun Joo Lee, Jinwoo Lee, Seung-Young Oh
Acute and Critical Care.2020; 35(2): 77. CrossRef - Current State and Strategy for Establishing a Digitally Innovative Hospital: Memorial Review Article for Opening of Yongin Severance Hospital
Soo-Jeong Kim, Ji Woong Roh, Sungwon Kim, Jin Young Park, Donghoon Choi
Yonsei Medical Journal.2020; 61(8): 647. CrossRef - Bleeding management after implementation of the Hemorrhage Code (Code H) at the Hospital Israelita Albert Einstein, São Paulo, Brazil
Michele Jaures, Neila Maria Marques Negrini Pigatti, Roseny dos Reis Rodrigues, Fernanda Paulino Fernandes, João Carlos de Campos Guerra
Einstein (São Paulo).2020;[Epub] CrossRef - Management of post-cardiac arrest syndrome
Youngjoon Kang
Acute and Critical Care.2019; 34(3): 173. CrossRef - Effect of a rapid response system on code rates and in-hospital mortality in medical wards
Hong Yeul Lee, Jinwoo Lee, Sang-Min Lee, Sulhee Kim, Eunjin Yang, Hyun Joo Lee, Hannah Lee, Ho Geol Ryu, Seung-Young Oh, Eun Jin Ha, Sang-Bae Ko, Jaeyoung Cho
Acute and Critical Care.2019; 34(4): 246. CrossRef - Evidence revealed the effects of rapid response system
Jae Hwa Cho
Acute and Critical Care.2019; 34(4): 282. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite