Pneumothorax Caused by Delayed Tracheal Rupture in a Pediatric Patient with Acute Respiratory Distress Syndrome
Article information

Tracheal rupture is a potentially lethal complication of endotracheal intubation [1-3] and usually occurs shortly after intubation [4]. Such rupture presents as a linear tear and is caused by movement of an over-inflated cuff or stylet [5]. Herein, we describe a case of pneumothorax caused by tracheal rupture after 30 days of intubation. A previously healthy 8-year-old boy was admitted to the pediatric intensive care unit for severe acute respiratory distress syndrome. The patient was treated with mechanical ventilation and extracorporeal membrane oxygenation. Cuff pressure was managed between 20 to 30 cmH2O, and the endotracheal tube was not changed before extubation. On hospital day 30, extubation was perfomred, and spontaneous breathing was noted. On the same day, massive pneumothorax was developed and was not controlled by chest tubes. Computed tomography showed a new lesion on the trachea (Figure 1), and bronchoscopy showed an oval ischemic lesion surrounded by a C-shaped tear (Figure 2). Since the position and size of the ischemic lesion were similar to those of the cuff, we suspected that prolonged cuff pressure created ischemia, and active breathing tore the weak margin. Managing cuff pressure in children requires high caution, and suspicion of tracheal rupture should be considered as a cause of pneumothorax.
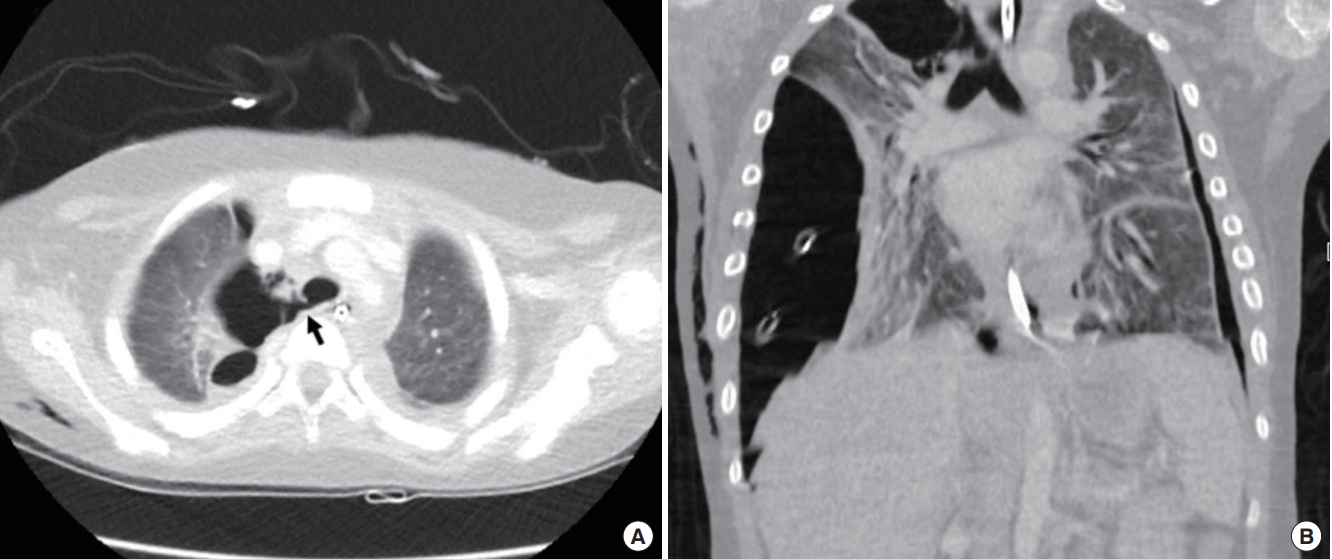
Chest computed tomography with post-contrast views. (A) A black arrow marks a 4-mm tracheal tear at the level of T3-4. Air collection is also presented on sagittal view. (B) Tracheal rupture appears above the carina on the right side.
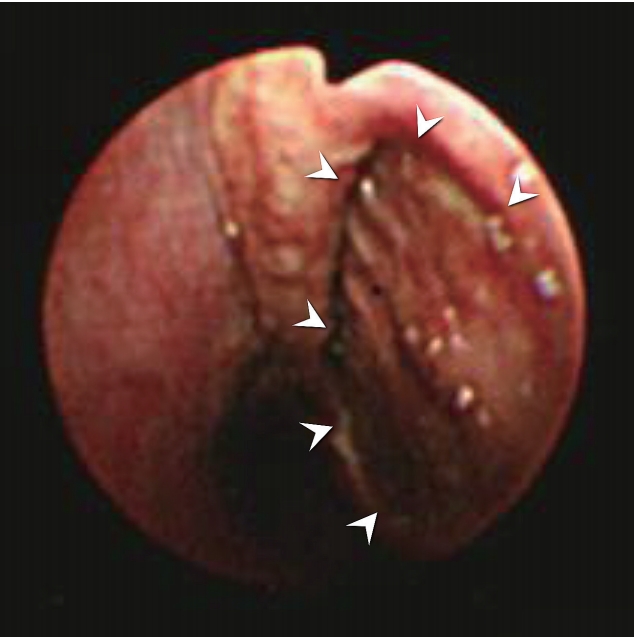
Bronchoscopic findings. A C-shaped tracheal rupture (white arrowheads) around the oval ischemic lesion at the posterior membrane of the lower third of the trachea.
Notes
CONFLICT OF INTEREST No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: MJ, JHC, AYC, MK, JC. Data curation: MJ, JHC. Writing original draft: MJ, AYC. Writing-review & editing: MK, JHC, JC.