Articles
- Page Path
- HOME > Acute Crit Care > Volume 34(3); 2019 > Article
- Original Article Characteristics, management and clinical outcomes of patients with sepsis: a multicenter cohort study in Korea
-
Kyeongman Jeon1
 , Soo Jin Na1, Dong Kyu Oh2, Sunghoon Park3, Eun Young Choi4, Seok Chan Kim5, Gil Myeong Seong6, Jeongwon Heo7, Youjin Chang8, Won Gun Kwack9, Byung Ju Kang10, Won-Il Choi11, Kyung Chan Kim12, So Young Park13, Sang Hyun Kwak14, Yoon Mi Shin15, Heung Bum Lee16, So Hee Park17, Jae Hwa Cho18, Beongki Kim19, Chae‐Man Lim2,
, Soo Jin Na1, Dong Kyu Oh2, Sunghoon Park3, Eun Young Choi4, Seok Chan Kim5, Gil Myeong Seong6, Jeongwon Heo7, Youjin Chang8, Won Gun Kwack9, Byung Ju Kang10, Won-Il Choi11, Kyung Chan Kim12, So Young Park13, Sang Hyun Kwak14, Yoon Mi Shin15, Heung Bum Lee16, So Hee Park17, Jae Hwa Cho18, Beongki Kim19, Chae‐Man Lim2, -
Acute and Critical Care 2019;34(3):179-191.
DOI: https://doi.org/10.4266/acc.2019.00514
Published online: July 1, 2019
1Department of Critical Care Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
2Department of Pulmonary and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
3Department of Pulmonary, Allergy and Critical Care Medicine, Hallym University Sacred Heart Hospital, Anyang, Korea
4Division of Respiratory and Critical Care Medicine, Department of Internal Medicine, Yeungnam University Medical Center, Daegu, Korea
5Division of Pulmonary and Critical Care Medicine, Department of Medicine, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
6Department of Internal Medicine, Jeju National University Hospital, Jeju National University School of Medicine, Jeju, Korea
7Department of Internal Medicine, Kangwon National University Hospital, Chuncheon, Korea
8Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Inje University Sanggye Paik Hospital, Seoul, Korea
9Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Kyung Hee University Hospital, Seoul, Korea
10Department of Internal Medicine, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea
11Department of Medicine, Keimyung University Dongsan Medical Center, Daegu, Korea
12Department of Internal Medicine, Daegu Catholic University Medical Center, Daegu Catholic University College of Medicine, Daegu, Korea
13Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Chungnam National University Hospital, Daejeon, Korea
14Department of Anesthesiology, Chonnam National University Hospital, Gwangju, Korea
15Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Chungbuk National University Hospital, Cheongju, Korea
16Department of Internal Medicine, Research Center for Pulmonary Disorders, Chonbuk National University Medical School, Jeonju, Korea
17Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Inje University Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea
18Department of Internal Medicine, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea
19Division of Pulmonology, Department of Internal Medicine, Korea University Ansan Hospital, Ansan, Korea
- Corresponding author Chae-Man Lim Department of Pulmonary and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpa-gu, Seoul 05505, Korea Tel: +82-2-3010-4710 Fax: +82-2-2045-4039 E-mail: cmlim@amc.seoul.kr
- *Current affiliation: Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Ewha Womans University Seoul Hospital, Seoul, Korea
Copyright © 2019 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background
- Mortality rates associated with sepsis have increased progressively in Korea, but domestic epidemiologic data remain limited. The objective of this study was to investigate the characteristics, management and clinical outcomes of sepsis patients in Korea.
-
Methods
- This study is a multicenter retrospective cohort study. A total of 64,021 adult patients who visited an emergency department (ED) within one of the 19 participating hospitals during a 1-month period were screened for eligibility. Among these, patients diagnosed with sepsis based on the third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) were included in the study.
-
Results
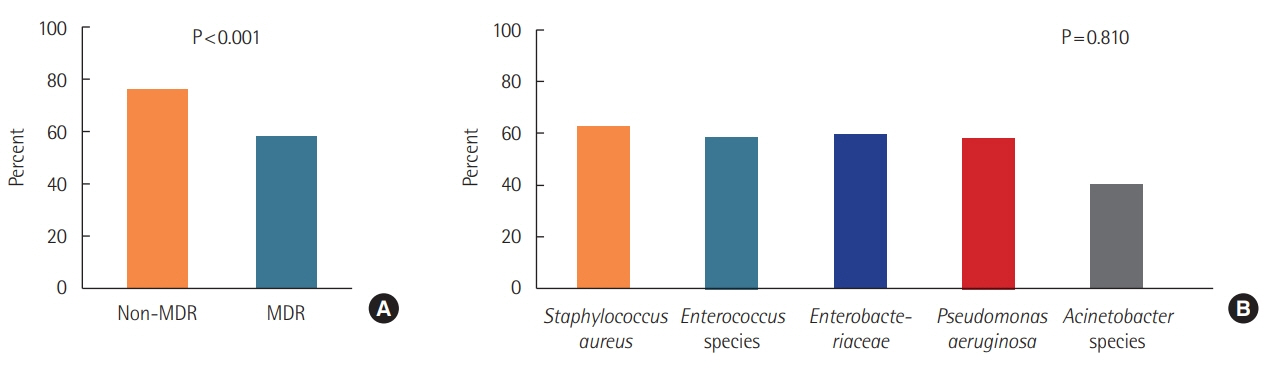
- Using the Sepsis-3 criteria, 977 sepsis patients were identified, among which 36.5% presented with septic shock. The respiratory system (61.8%) was the most common site of infection. The pathogen involved was identified in 444 patients (45.5%) and multi-drug resistance (MDR) pathogens were isolated in 171 patients. Empiric antibiotic therapy was appropriate in 68.6% of patients, but the appropriateness was significantly reduced in infections associated with MDR pathogens as compared with non-MDR pathogens (58.8% vs. 76.0%, P<0.001). Hospital mortality was 43.2% and 18.5% in sepsis patients with and without shock, respectively. Of the 703 patients who survived to discharge, 61.5% were discharged to home and 38.6% were transferred to other hospitals or facilities.
-
Conclusions
- This study found the prevalence of sepsis in adult patients visiting an ED in Korea was 1.5% (15.2/1,000 patients). Patients with sepsis, especially septic shock, had a high mortality and were often referred to step-down centers after acute and critical care.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
DISCUSSION
KEY MESSAGES
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conceptualization: KJ, SHP, CML. Methodology: KJ, SHP, CML. Investigation: KJ, DKO, SP, EYC, SCK, GMS, JH, YC, WGK, BJK, WIC, KCK, SYP, SHK, YMS, HBL, SHP, JHC, BK. Formal analysis: KJ, SJN. Writing – original draft: KJ, SJN. Writing – review and editing: all authors.
NOTES
Acknowledgments
Values are presented as median (interquartile range) or number (%).
SOFA: Sequential Organ Failure Assessment; AST: aspartate aminotransferase; ALT: alanine aminotransferase; INR: international normalized ratio; PaCO2: partial pressure of carbon dioxide in arterial blood; PaO2: partial pressure of oxygen in arterial blood; BNP: brain natriuretic peptide.
| Variable | Overall (n=977) | Sepsis (n=620) | Septic shock (n=357) | P-value |
|---|---|---|---|---|
| Classification of infection | ||||
| Microbiologically documented infection | 444 (45.5) | 258 (41.6) | 186 (52.1) | 0.002 |
| Clinically documented infection | 430 (44.0) | 293 (47.3) | 137 (38.4) | 0.007 |
| Possible infection | 103 (10.5) | 69 (11.1) | 34 (9.5) | 0.431 |
| Site of infection | ||||
| Respiratory tract | 604 (61.8) | 411 (66.3) | 193 (54.1) | <0.001 |
| Abdominal cavity | 161 (16.5) | 83 (13.4) | 78 (21.9) | <0.001 |
| Urinary tract | 122 (12.5) | 85 (13.7) | 37 (10.4) | 0.128 |
| Skin/soft tissue | 27 (2.8) | 17 (2.7) | 10 (2.8) | 0.957 |
| Catheter-related | 7 (0.7) | 3 (0.5) | 4 (1.1) | 0.266 |
| Neurological | 7 (0.7) | 5 (0.8) | 2 (0.6) | >0.999 |
| Infections without a clear primary site of infection | 49 (5.0) | 16 (2.6) | 33 (9.2) | <0.001 |
| Type of infection | 0.338 | |||
| Community-acquired infection | 790 (80.9) | 507 (81.8) | 283 (79.3) | |
| Hospital-acquired infection | 187 (19.1) | 113 (18.2) | 74 (20.7) | |
| Cultured pathogena | ||||
| Respiratory | 147 (33.4) | 93 (37.7) | 52 (27.2) | 0.021 |
| Blood | 186 (42.3) | 87 (35.2) | 104 (54.5) | <0.001 |
| Urine | 66 (15.0) | 48 (19.4) | 18 (9.4) | 0.004 |
| Catheter | 2 (0.5) | 0 | 2 (1.1) | 0.190 |
| Others | 34 (7.7) | 19 (7.7) | 15 (7.9) | 0.950 |
| Multi-drug resistance pathogen | 171 (17.8) | 96 (15.8) | 75 (21.1) | 0.039 |
| Staphylococcus aureus | 36 (21.1) | 17 (17.7) | 19 (25.3) | |
| Enterococcus species | 13 (7.6) | 6 (6.3) | 7 (9.3) | |
| Enterobacteriaceae | 86 (50.3) | 52 (54.2) | 34 (45.3) | |
| Pseudomonas aeruginosa | 18 (10.5) | 15 (15.6) | 3 (4.0) | |
| Acinetobacter species | 9 (5.3) | 2 (2.1) | 7 (9.3) | |
| Clostridium perfringens | 1 (0.6) | 0 | 1 (1.3) | |
| No data | 8 (4.7) | 4 (4.2) | 4 (5.3) |
| Variable | Overall (n=977) | Sepsis (n=620) | Septic shock (n=357) | P-value |
|---|---|---|---|---|
| Initial empirical antibiotics | ||||
| Beta-lactam | 837 (87.5) | 534 (88.7) | 303 (85.4) | 0.130 |
| Fluroquinolone | 295 (30.8) | 189 (31.4) | 106 (29.9) | 0.619 |
| Aminoglycoside | 12 (1.3) | 7 (1.2) | 5 (1.4) | 0.769 |
| Glycopeptide | 86 (9.0) | 38 (6.3) | 48 (13.5) | <0.001 |
| Colistin | 1 (0.1) | 0 | 1 (0.3) | 0.371 |
| Carbapenem | 73 (7.6) | 27 (4.5) | 46 (13.0) | <0.001 |
| Macrolide | 96 (10.0) | 75 (12.5) | 21 (5.9) | 0.001 |
| Others | 75 (15.2) | 35 (11.2) | 40 (22.9) | 0.001 |
| Combination antibiotic therapy | 484 (50.5) | 293 (48.5) | 191 (53.8) | 0.113 |
| Appropriateness of initial antibiotics | ||||
| Appropriate | 670 (68.6) | 420 (67.9) | 250 (70.0) | 0.480 |
| Inappropriate | 172 (17.6) | 103 (16.6) | 69 (19.3) | 0.288 |
| Not available | 134 (13.7) | 96 (15.5) | 38 (10.6) | 0.033 |
| Nonsurgical source control measure implemented | 132 (13.5) | 71 (11.5) | 61 (17.1) | 0.013 |
| Removal of infected intravascular or other catheters | 35 (4.2) | 11 (2.1) | 24 (7.7) | <0.001 |
| Insertion of percutaneous drain catheters | 86 (10.3) | 49 (9.3) | 37 (11.9) | 0.227 |
| Pleural | 33 (38.4) | 16 (32.7) | 17 (46.0) | |
| Hepatobiliary | 29 (33.7) | 18 (36.7) | 11 (29.7) | |
| Peritoneum | 10 (11.6) | 6 (12.2) | 4 (10.8) | |
| Others | 14 (16.3) | 9 (18.4) | 5 (13.5) | |
| Other nonsurgical source control measure | 20 (2.4) | 16 (3.0) | 4 (1.3) | 0.109 |
| Surgical source control | 20 (2.1) | 9 (1.5) | 11 (3.2) | 0.075 |
| Intensive care unit admission | 294 (33.9) | 111 (20.6) | 183 (55.5) | <0.001 |
| Treatment during intensive care unit staya | ||||
| Mechanical ventilation | 182 (63.9) | 68 (58.6) | 114 (67.5) | 0.127 |
| Renal replacement therapy | 70 (24.6) | 25 (21.6) | 45 (26.6) | 0.328 |
| Extracorporeal membrane oxygenation | 12 (4.2) | 5 (4.3) | 7 (4.1) | >0.999 |
| Hemoperfusion | 22 (7.7) | 4 (3.5) | 18 (10.7) | 0.025 |
Values are presented as median (interquartile range) or number (%).
SOFA: Sequential Organ Failure Assessment; AST: aspartate aminotransferase; ALT: alanine aminotransferase; INR: international normalized ratio; PaCO2: partial pressure of carbon dioxide in arterial blood; PaO2: partial pressure of oxygen in arterial blood; BNP: brain natriuretic peptide.
|
Univariable |
Multivariable |
|||
|---|---|---|---|---|
| OR (95% CI) | P-value | Adjusted OR (95% CI) | P-value | |
| Age (yr) | 1.01 (1.00–1.02) | 0.061 | 1.02 (1.01–1.03) | 0.004 |
| Initial SOFA score | 1.17 (1.13–1.22) | <0.001 | 1.14 (1.08–1.19) | <0.001 |
| Septic shock | 3.35 (2.50–4.49) | <0.001 | 2.56 (1.80–3.62) | <0.001 |
| Solid or hematological malignancy | 1.34 (1.00–1.80) | 0.054 | 1.84 (1.31–2.58) | <0.001 |
| Site of infectiona | ||||
| Abdominal | 0.78 (0.53–1.16) | 0.221 | 0.66 (0.43–1.02) | 0.060 |
| Urinary | 0.34 (0.19–0.58) | <0.001 | 0.30 (0.17–0.54) | <0.001 |
| Othersb | 0.62 (0.37–1.05) | 0.078 | 0.37 (0.20–0.67) | 0.001 |
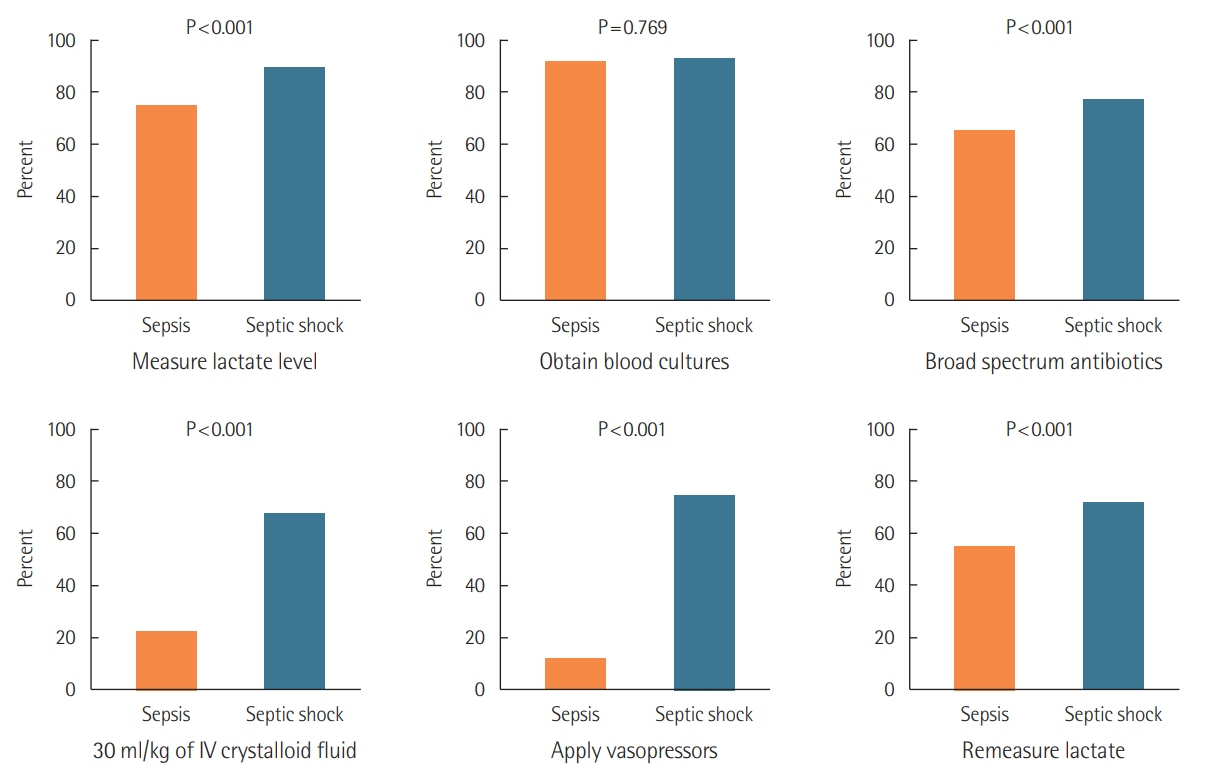
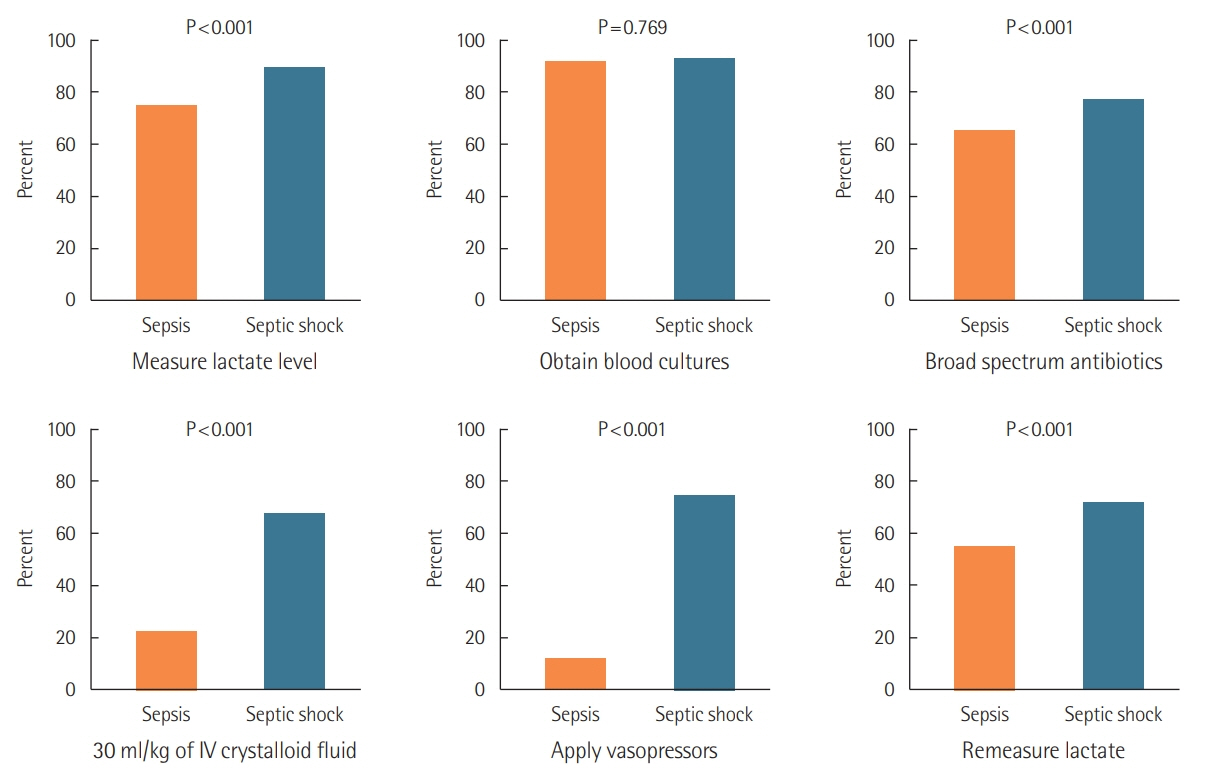
| Measure lactate level | 1.69 (1.14–2.50) | 0.008 | 1.11 (0.72–1.71) | 0.649 |
| Obtain blood cultures | 1.00 (0.6.0–1.68) | 0.986 | 0.89 (0.50–1.57) | 0.677 |
| Broad spectrum antibiotics | 1.54 (1.11–2.12) | 0.009 | 1.17 (0.81–1.69) | 0.413 |
| Crystalloid fluid | 1.95 (1.47–2.60) | <0.001 | 1.02 (0.71–1.46) | 0.905 |
- 1. Fleischmann C, Scherag A, Adhikari NK, Hartog CS, Tsaganos T, Schlattmann P, et al. Assessment of global incidence and mortality of hospital-treated sepsis: current estimates and limitations. Am J Respir Crit Care Med 2016;193:259-72.ArticlePubMed
- 2. Iwashyna TJ, Ely EW, Smith DM, Langa KM. Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA 2010;304:1787-94.ArticlePubMedPMC
- 3. Reinhart K, Daniels R, Kissoon N, Machado FR, Schachter RD, Finfer S. Recognizing sepsis as a global health priority: a WHO resolution. N Engl J Med 2017;377:414-7.ArticlePubMed
- 4. Vincent JL, Marshall JC, Namendys-Silva SA, François B, Martin-Loeches I, Lipman J, et al. Assessment of the worldwide burden of critical illness: the intensive care over nations (ICON) audit. Lancet Respir Med 2014;2:380-6.ArticlePubMed
- 5. Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012. JAMA 2014;311:1308-16.ArticlePubMed
- 6. Vincent JL, Rello J, Marshall J, Silva E, Anzueto A, Martin CD, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA 2009;302:2323-9.ArticlePubMed
- 7. Choe YJ, Choe SA, Cho SI. Trends in infectious disease mortality, South Korea, 1983-2015. Emerg Infect Dis 2018;24:320-7.ArticlePubMedPMC
- 8. Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016;315:801-10.ArticlePubMedPMC
- 9. Magiorakos AP, Srinivasan A, Carey RB, Carmeli Y, Falagas ME, Giske CG, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect 2012;18:268-81.ArticlePubMed
- 10. Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med 2017;43:304-77.ArticlePubMedPDF
- 11. Levy MM, Evans LE, Rhodes A. The Surviving Sepsis Campaign Bundle: 2018 update. Intensive Care Med 2018;44:925-8.ArticlePubMed
- 12. Sakr Y, Jaschinski U, Wittebole X, Szakmany T, Lipman J, Ñamendys-Silva SA, et al. Sepsis in intensive care unit patients: worldwide data from the intensive care over nations audit. Open Forum Infect Dis 2018;5:ofy313. ArticlePubMedPMCPDF
- 13. Lee CC, Yo CH, Lee MG, Tsai KC, Lee SH, Chen YS, et al. Adult sepsis: a nationwide study of trends and outcomes in a population of 23 million people. J Infect 2017;75:409-19.ArticlePubMed
- 14. Zhou J, Tian H, Du X, Xi X, An Y, Duan M, et al. Populationbased epidemiology of sepsis in a subdistrict of Beijing. Crit Care Med 2017;45:1168-76.ArticlePubMed
- 15. Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med 2001;29:1303-10.ArticlePubMed
- 16. Abe T, Ogura H, Shiraishi A, Kushimoto S, Saitoh D, Fujishima S, et al. Characteristics, management, and in-hospital mortality among patients with severe sepsis in intensive care units in Japan: the FORECAST study. Crit Care 2018;22:322. ArticlePubMedPMCPDF
- 17. Wang HE, Jones AR, Donnelly JP. Revised national estimates of emergency department visits for sepsis in the United States. Crit Care Med 2017;45:1443-9.ArticlePubMedPMC
- 18. Phua J, Koh Y, Du B, Tang YQ, Divatia JV, Tan CC, et al. Management of severe sepsis in patients admitted to Asian intensive care units: prospective cohort study. BMJ 2011;342:d3245. ArticlePubMedPMC
- 19. Park DW, Chun BC, Kim JM, Sohn JW, Peck KR, Kim YS, et al. Epidemiological and clinical characteristics of communityacquired severe sepsis and septic shock: a prospective observational study in 12 university hospitals in Korea. J Korean Med Sci 2012;27:1308-14.ArticlePubMedPMC
- 20. Lee JY, Yoo CG, Kim HJ, Jung KS, Yoo KH. Disease burden of pneumonia in Korean adults aged over 50 years stratified by age and underlying diseases. Korean J Intern Med 2014;29:764-73.ArticlePubMedPMCPDF
- 21. Kim HJ, Choi SM, Lee J, Park YS, Lee CH, Yim JJ, et al. Respiratory virus of severe pneumonia in South Korea: prevalence and clinical implications. PLoS One 2018;13:e0198902.ArticlePubMedPMC
- 22. Zilberberg MD, Shorr AF, Micek ST, Vazquez-Guillamet C, Kollef MH. Multi-drug resistance, inappropriate initial antibiotic therapy and mortality in Gram-negative severe sepsis and septic shock: a retrospective cohort study. Crit Care 2014;18:596. ArticlePubMedPMCPDF
- 23. Gandra S, Tseng KK, Arora A, Bhowmik B, Robinson ML, Panigrahi B, et al. The mortality burden of multidrug-resistant pathogens in India: a retrospective, observational study. Clin Infect Dis 2019;69:563-70.ArticlePDF
References
Figure & Data
References
Citations
- Early Prediction of Mortality for Septic Patients Visiting Emergency Room Based on Explainable Machine Learning: A Real-World Multicenter Study
Sang Won Park, Na Young Yeo, Seonguk Kang, Taejun Ha, Tae-Hoon Kim, DooHee Lee, Dowon Kim, Seheon Choi, Minkyu Kim, DongHoon Lee, DoHyeon Kim, Woo Jin Kim, Seung-Joon Lee, Yeon-Jeong Heo, Da Hye Moon, Seon-Sook Han, Yoon Kim, Hyun-Soo Choi, Dong Kyu Oh, S
Journal of Korean Medical Science.2024;[Epub] CrossRef - Deficits in blood culture collection in the emergency department if sepsis is suspected: results of a retrospective cohort study
Charlotte Berninghausen, Frank Schwab, Alexander Gropmann, Bernd A. Leidel, Rajan Somasundaram, Lydia Hottenbacher, Petra Gastmeier, Sonja Hansen
Infection.2024;[Epub] CrossRef - Pre-Sepsis Length of Hospital Stay and Mortality: A Nationwide Multicenter Cohort Study
Joong-Yub Kim, Hong Yeul Lee, Jinwoo Lee, Dong Kyu Oh, Su Yeon Lee, Mi Hyeon Park, Chae-Man Lim, Sang-Min Lee
Journal of Korean Medical Science.2024;[Epub] CrossRef - Platelet indices in critically ill septic patients as a predictor of mortality
Rehab Salah Taha, Mohamed Elsayed Afandy, Abdelaziz Hamid Elbadawi, Mohamed Samir Abd El Ghafar
Egyptian Journal of Anaesthesia.2023; 39(1): 56. CrossRef - Antibiogram of Multidrug-Resistant Bacteria Based on Sepsis Onset Location in Korea: A Multicenter Cohort Study
Hyung-Jun Kim, Dong Kyu Oh, Sung Yoon Lim, Young-Jae Cho, Sunghoon Park, Gee Young Suh, Chae-Man Lim, Yeon Joo Lee
Journal of Korean Medical Science.2023;[Epub] CrossRef - HYPOTENSION AT THE TIME OF SEPSIS RECOGNITION IS NOT ASSOCIATED WITH INCREASED MORTALITY IN SEPSIS PATIENTS WITH NORMAL LACTATE LEVELS
Ji Hwan Kim, Yong Kyun Kim, Dong Kyu Oh, Kyeongman Jeon, Ryoung-Eun Ko, Gee Young Suh, Sung Yun Lim, Yeon Joo Lee, Young-Jae Cho, Mi-Hyeon Park, Sang-Bum Hong, Chae-Man Lim, Sunghoon Park
Shock.2023; 59(3): 360. CrossRef - Mortality among adult patients with sepsis and septic shock in Korea: a systematic review and meta-analysis
Myeong Namgung, Chiwon Ahn, Yeonkyung Park, Il-Youp Kwak, Jungguk Lee, Moonho Won
Clinical and Experimental Emergency Medicine.2023; 10(2): 157. CrossRef - Effects of prior antiplatelet and/or nonsteroidal anti-inflammatory drug use on mortality in patients undergoing abdominal surgery for abdominal sepsis
Se Hun Kim, Ki Hoon Kim
Surgery.2023; 174(3): 611. CrossRef - Clinical effects of bacteremia in sepsis patients with community-acquired pneumonia
Tae Wan Kim, Se-Uk Lee, Boram Park, Kyeongman Jeon, Sunghoon Park, Gee Young Suh, Dong Kyu Oh, Soo Yeon Lee, Mi Hyeon Park, Haein Lee, Chae-man Lim, Ryoung-Eun Ko, Sang-Bum Hong, Suk-Kyung Hong, Yeon Joo Lee, Young-Jae Cho, Sung Yoon Lim, Jeongwon Heo, Ja
BMC Infectious Diseases.2023;[Epub] CrossRef - Current status of treatment of acute respiratory failure in Korea
Yong Jun Choi, Jae Hwa Cho
Journal of the Korean Medical Association.2022; 65(3): 124. CrossRef - Clinical Characteristics and Outcomes of Neutropenic Sepsis: A Multicenter Cohort Study
Soo Jin Na, Dong Kyu Oh, Sunghoon Park, Yeon Joo Lee, Sang-Bum Hong, Mi-Hyun Park, Ryoung-Eun Ko, Chae-Man Lim, Kyeongman Jeon
Shock.2022; 57(5): 659. CrossRef - Mortality of patients with hospital-onset sepsis in hospitals with all-day and non-all-day rapid response teams: a prospective nationwide multicenter cohort study
Dong-gon Hyun, Su Yeon Lee, Jee Hwan Ahn, Jin Won Huh, Sang-Bum Hong, Younsuck Koh, Chae-Man Lim, Dong Kyu Oh, Gee Young Suh, Kyeongman Jeon, Ryoung-Eun Ko, Young-Jae Cho, Yeon Joo Lee, Sung Yoon Lim, Sunghoon Park, Jeongwon Heo, Jae-myeong Lee, Kyung Cha
Critical Care.2022;[Epub] CrossRef - Clinical outcomes and prognostic factors of patients with sepsis caused by intra-abdominal infection in the intensive care unit: a post-hoc analysis of a prospective cohort study in Korea
Chan Hee Park, Jeong Woo Lee, Hak Jae Lee, Dong Kyu Oh, Mi Hyeon Park, Chae-Man Lim, Suk-Kyung Hong, Chae-Man Lim, Sang-Bum Hong, Dong Kyu Oh, Gee Young Suh, Kyeongman Jeon, Ryoung-Eun Ko, Young-Jae Cho, Yeon Joo Lee, Sung Yoon Lim, Sunghoon Park, Chae-Ma
BMC Infectious Diseases.2022;[Epub] CrossRef - Sepsis in the XXI Century: Etiology, Risk Factors, Epidemiological Features, Complications, Prevention
L. I. Gomanova, A. Y. Brazhnikov
Epidemiology and Vaccinal Prevention.2021; 20(3): 107. CrossRef - Characteristics, Management, and Clinical Outcomes of Patients with Hospital-Acquired and Ventilator-Associated Pneumonia: A Multicenter Cohort Study in Korea
Ryoung-Eun Ko, Kyung Hoon Min, Sang-Bum Hong, Ae-Rin Baek, Hyun-Kyung Lee, Woo Hyun Cho, Changhwan Kim, Youjin Chang, Sung-Soon Lee, Jee Youn Oh, Heung Bum Lee, Soohyun Bae, Jae Young Moon, Kwang Ha Yoo, Kyeongman Jeon
Tuberculosis and Respiratory Diseases.2021; 84(4): 317. CrossRef - Clinical Usefulness of Red Cell Distribution Width/Albumin Ratio to Discriminate 28-Day Mortality in Critically Ill Patients with Pneumonia Receiving Invasive Mechanical Ventilation, Compared with Lacate/Albumin Ratio: A Retrospective Cohort Study
Jong Hwan Jeong, Manbong Heo, Seung Jun Lee, Yi Yeong Jeong, Jong Deog Lee, Jung-Wan Yoo
Diagnostics.2021; 11(12): 2344. CrossRef - Review of 20 Years of Continuous Quality Improvement of a Rapid Response System, at Four Institutions, to Identify Key Process Responsible for Its Success
Mary Anne Vandegrift, Robert Granata, Vicken Y. Totten, John Kellett, Frank Sebat
Critical Care Explorations.2021; 3(8): e0448. CrossRef - An Update on Sepsis Biomarkers
Mi-Hee Kim, Jung-Hyun Choi
Infection & Chemotherapy.2020; 52(1): 1. CrossRef - Normothermia in Patients With Sepsis Who Present to Emergency Departments Is Associated With Low Compliance With Sepsis Bundles and Increased In-Hospital Mortality Rate*
Sunghoon Park, Kyeongman Jeon, Dong Kyu Oh, Eun Young Choi, Gil Myeong Seong, Jeongwon Heo, Youjin Chang, Won Gun Kwack, Byung Ju Kang, Won-Il Choi, Kyung Chan Kim, So Young Park, Yoon Mi Shin, Heung Bum Lee, So Hee Park, Seok Chan Kim, Sang Hyun Kwak, Ja
Critical Care Medicine.2020; 48(10): 1462. CrossRef - Prevention of sepsis in an aging society
Youngjoon Kang
Acute and Critical Care.2019; 34(3): 221. CrossRef - Optimal antimicrobial therapy and antimicrobial stewardship in sepsis and septic shock
Hyeri Seok, Dae Won Park
Journal of the Korean Medical Association.2019; 62(12): 638. CrossRef - Sepsis
Yunghee Lee, Young-Jae Cho
The Korean Journal of Medicine.2019; 94(6): 495. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite