Abstract
-
Background:
- It has been suggested that a high-flow nasal cannula (HFNC) could help to remove carbon dioxide (CO2) from anatomical dead spaces, but evidence to support that is lacking. The objective of this study was to elucidate whether use of an HFNC could reduce the arterial partial pressure of CO2 (PaCO2) in patients with acute hypercapnic respiratory failure who are receiving conventional oxygen (O2) therapy.
-
Methods:
- A propensity score-matched observational study was conducted to evaluate patients treated with an HFNC for acute hypercapnic respiratory failure from 2015 to 2016. The hypercapnia group was defined as patients with a PaCO2 >50 mm Hg and arterial pH <7.35.
-
Results:
- Eighteen patients in the hypercapnia group and 177 patients in the nonhypercapnia group were eligible for the present study. Eighteen patients in each group were matched by propensity score. Decreased PaCO2 and consequent pH normalization over time occurred in the hypercapnia group (P=0.002 and P=0.005, respectively). The initial PaCO2 level correlated linearly with PaCO2 removal after the use of an HFNC (R2=0.378, P=0.010). The fraction of inspired O2 used in the intensive care unit was consistently higher for 48 hours in the nonhypercapnia group. Physiological parameters such as respiratory rate and arterial partial pressure of O2 improved over time in both groups.
-
Conclusions:
- Physiological parameters can improve after the use of an HFNC in patients with acute hypercapnic respiratory failure given low-flow O2 therapy via a facial mask. Further studies are needed to identify which hypercapnic patients might benefit from an HFNC.
-
Keywords: hypercapnia; oxygen inhalation therapy; respiratory insufficiency
INTRODUCTION
The high-flow nasal cannula (HFNC) has several physiological benefits, one of which is to facilitate carbon dioxide (CO2) washout from the airway system [1-3]. Although the theoretical background for CO2 “sweeping” has been explained in various ways, previous studies have consistently reported improved ventilation after the use of an HFNC [4]. For example, breathing frequency and minute ventilation decrease without changing the arterial partial pressure of CO2 (PaCO2), which makes respiratory ventilation more efficient by decreasing the dead space [5,6]. Some researchers have suggested that reducing the overall dead space in the airway system can improve respiratory ventilation and ultimately help to remove CO2 [7,8]. Others have reported that the endexpiratory lung volume increases after the application of an HFNC, which might result in collapsed alveoli and increase gas flow [9,10]. However, the guidelines for managing acute hypercapnic respiratory failure recommend noninvasive ventilation (NIV) as the treatment of choice and suggest that an HFNC should not be used because of a lack of evidence for the benefits and the possibility of respiratory suppression [11,12]. Although intolerance or lung injury caused by the application of bilevel pressure has frequently been reported in patients treated with noninvasive or invasive ventilation, no alternative noninvasive options have been suggested [13,14].
Recent clinical trials have reported the benefits of using an HFNC to treat patients with obstructive lung disease or hypercapnia. The short-term application of an HFNC decreases the transcutaneous CO2 level and improves other physiological parameters in patients who require long-term oxygen (O2) therapy to treat stable chronic obstructive pulmonary disease (COPD) [15]. For example, the PaCO2 level decreased more as the rate of gas flow in an HFNC increased in stable COPD patients [16]. In another study, HFNCs allowed patients with severe COPD to increase their exercise capacity without retaining CO2 [17]. Short-term use of an HFNC causes a decrease in transcutaneous CO2 levels even during an acute exacerbation of COPD [18]. Most of the previous studies on the use of an HFNC in treating hypercapnia have focused exclusively on relatively stable patients without considering patients with unstable hypercapnic status.
We conducted the present study to clarify whether, compared with nonhypercapnic patients, hypercapnic patients exhibit a tendency for CO2 retention or CO2 removal after the use of an HFNC. Our aim in the present study was to elucidate how physiological parameters change in relation to the initial PaCO2 level after the use of an HFNC in patients with acute respiratory failure given a facial mask for O2 therapy.
MATERIALS AND METHODS
Study Population and Study Design
This propensity score-matched cohort study was conducted by reviewing the electronic medical records in a tertiary teaching hospital. The study population comprised patients admitted to our hospital and given O2 therapy via an HFNC to manage acute respiratory failure between January 2015 and December 2016. The inclusion criteria were as follows: (1) the patient could breathe spontaneously without impaired mental status, (2) the patient was given O2 therapy with a facial mask before the application of an HFNC, (3) an HFNC was applied for at least 48 hours, (4) physiological parameters were measured continuously during HFNC use, and (5) the patient’s age >18 years. The exclusion criteria were any of the following conditions that could influence the targeted physiological parameters other than acute respiratory failure: (1) concurrent metabolic acidosis or alkalosis, (2) hemodialysis or peritoneal dialysis, (3) extracorporeal membrane oxygenation or extracorporeal CO2 removal, or (4) invasive or noninvasive mechanical ventilation.
The study population was classified into hypercapnia and nonhypercapnia groups. The hypercapnia group was defined as patients with acute hypercapnic respiratory failure, PaCO2 >50 mm Hg, and arterial pH <7.35 [11,19]. Both groups were given conventional O2 therapy with a facial mask for hypoxemia until an HFNC was applied.
We first reviewed the demographic characteristics (age, sex, body mass index, level of consciousness, declaration of a “do not resuscitate” or “do not intubate order,” department to which the patient was admitted, and comorbid chronic conditions). We recorded PaCO2, arterial pH, arterial partial pressure of O2 (PaO2), mean blood pressure, heart rate, respiratory rate, body temperature, O2 saturation, applied O2 flow rate, and applied fraction of inspired oxygen (FiO2). These parameters were checked at baseline and at 12, 24, and 48 hours after HFNC initiation. The variation in PaCO2 during the first 12 hours of HFNC use was recorded. The causes of acute respiratory failure were analyzed. The severity of each patient’s condition was assessed using the Acute Physiology and Chronic Health Evaluation (APACHE) II score, Sequential Organ Failure Assessment (SOFA) score, and the ratio of PaO2 to FiO2. For evaluation of clinical outcomes, we reviewed in-hospital mortality, survived days, and cause of death.
Assessment of Physiological and Clinical Outcomes
The primary aim of this study was to determine the variation in PaCO2 level before and after HFNC application for 48 hours. The secondary aim was to assess the associations between the change in PaCO2 during the first 12 hours of HFNC use and the initial level of PaCO2, respiratory rate, and O2 flow rate in the hypercapnia group. We also analyzed the changes in other physiological parameters such as pH, PaO2, mean blood pressure, heart rate, and respiratory rate over time. The in-hospital mortality rate within 28 days, mean survival time within 28 days, and cause of mortality were evaluated.
Statistics
Categorical variables were compared using Pearson’s chisquare test or Fisher’s exact test. Continuous variables were analyzed using the Student t-test, and the results are described using the mean and standard deviation. We created propensity scores using logistic regression analyses with demographic characteristics, underlying disease, results of blood tests except for arterial blood gas analysis (ABGA), cause of respiratory failure, initial vital signs, use of inotropes, and severity indexes as covariates. Propensity score matching was conducted at a one-to-one ratio. Repeated-measures analysis of variance in the propensity score–matched population was performed to identify significant changes in physiological parameters over time and differences between the hypercapnia and nonhypercapnia groups. Regression analysis with scatterplots was used to explain the relationships between CO2 washout and other factors. We used R ver. 3.4.0 (R Core Team 2017, Vienna, Austria) for our statistical analyses.
Ethics
The Institutional Review Board of Seoul National University Hospital examined and approved the protocol for our study and exempted us from the need for informed consent to access to the electronic medical records (IRB No. H-1704-085-665).
RESULTS
Baseline Characteristics of the Study Population
In total, 195 patients were eligible and subsequently classified into two groups: 18 patients in the hypercapnia group and 177 in the nonhypercapnia group (Figure 1). All patients were supplied with 11–15 L of O2 via a face mask before the application of an HFNC. In the analysis of the total study population, demographic features and the causes of respiratory failure showed significant heterogeneity between groups (Tables 1 and 2). Male sex and underlying cardiovascular disease were found more frequently in the hypercapnia group, and immune deficiency occurred in more patients in the nonhypercapnia group. The frequency of underlying chronic respiratory disease and acute exacerbation of COPD did not differ significantly between the two groups. A higher FiO2 was applied to the nonhypercapnia group, but the O2 flow rate was similar between groups. The initial vital signs, use of inotropes, and disease severity did not differ significantly between groups.
Eighteen patients in each group were matched one-to-one using the propensity score. The heterogeneity of the baseline characteristics and clinical features was adjusted and minimized, except for the targeted physiological parameters (Tables 3 and 4). The mean age was >70 years, and about 90% of the patients were men. More than half of the patients had a declared “do not resuscitate order,” and about one-third of the patients had a declared “do not intubate order.” Pneumonia, pulmonary edema, and acute exacerbation of COPD were the main causes of respiratory failure. The initial mean respiratory rate was about 30 per minute, and the mean oxygen saturation was about 90%. The mean APACHE II score was about 18, and mean SOFA score was about 6. In the ABGA, the hypercapnia group had a lower pH (7.31±0.09) and higher PaCO2 (61.5±15.1 mm Hg). A higher FiO2 was used with the HFNC in the nonhypercapnia group.
Physiological Parameters in the Propensity Score–Matched Patients
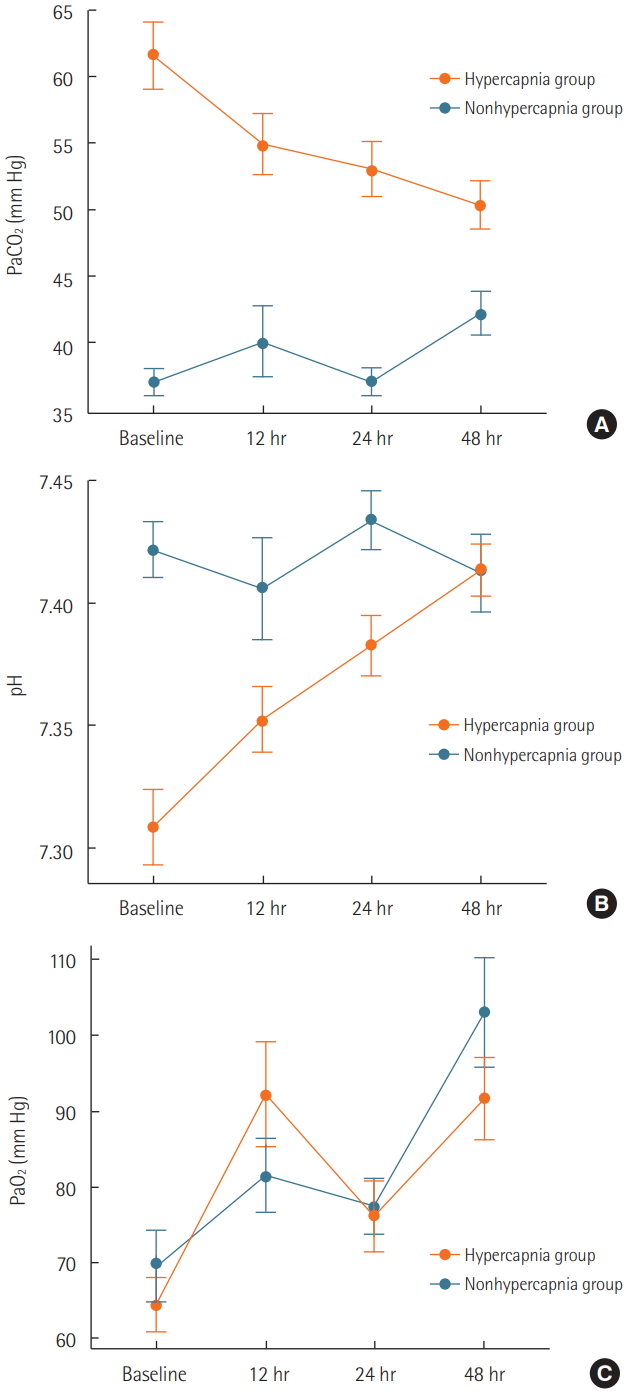
The PaCO2 level changed over time, but the pattern of change differed between patient groups (P=0.002 for the interaction of group and time) (Figure 2A). The PaCO2 level decreased over time (–11.2±12.7 mm Hg for 48 hours) in the hypercapnia group but tended to increase over time (5.2±12.2 mm Hg for 48 hours) in the nonhypercapnia group (P<0.001 for the interaction of group and time).
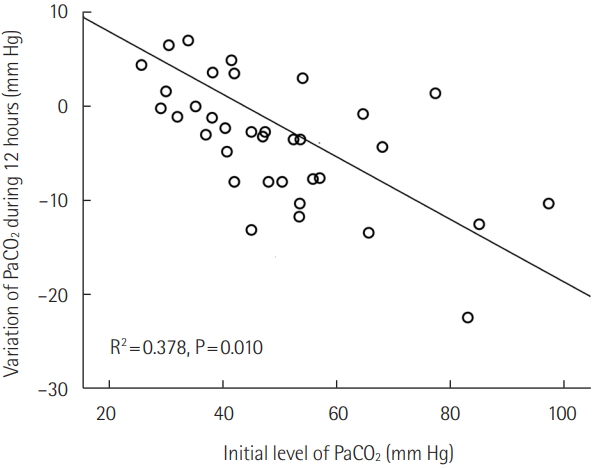
In the hypercapnia group, the variation in PaCO2 during the first 12 hours was related to the initial PaCO2 level; that is, more CO2 was washed out by the HFNC in patients with a higher PaCO2 (R2=0.378, P=0.010) (Figure 3). The decrease in PaCO2 was not related to the respiratory rate or O2 flow rate.
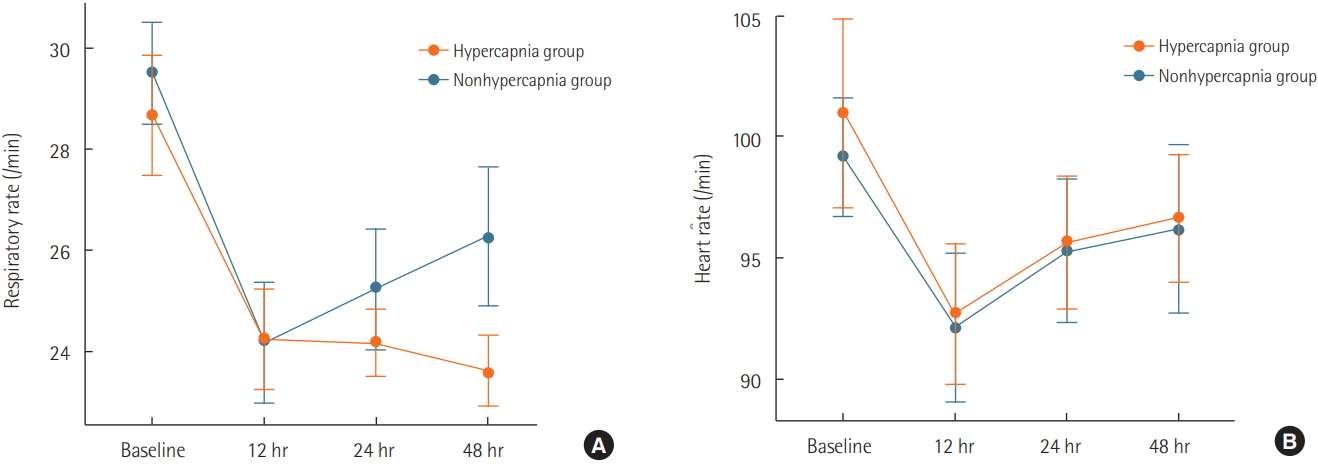
For pH, the pattern of change over time also differed between the groups (P=0.005 for the interaction of group and time) (Figure 2B). The pH increased with time in the hypercapnia group but remained constant in the nonhypercapnia group. PaO2 increased over time in both groups (P=0.001) (Figure 2C). All patients were supplied with 11–15 L of O2 via a facial mask before the application of an HFNC. The respiratory rate decreased similarly over time in both groups (P<0.001) (Figure 4A). The heart rate had decreased at 12 hours and then increased slightly at 24 and 48 hours, but the changes with time and differences between groups were not significant (Figure 4B). FiO2 did not change over time but did differ significantly between the groups: FiO2 was higher in the nonhypercapnia group (Figure 5A). The O2 flow rate increased for 24 hours and then decreased in the hypercapnia group, but it decreased slightly for 12 hours and then increased in the nonhypercapnia group (Figure 5B).
Ten patients (55.6%) in the hypercapnia group and 11 patients (61.1%) in the nonhypercapnia group died in the hospital (P=0.735) (Table 5). During the 28 days after the initiation of HFNC, the mean survival time was 16.9 days in the hypercapnia group and 17.2 days in the nonhypercapnia group (P=0.522). In the hypercapnia group, hypercapnia was aggravated in six patients, and intubation was performed in one patient 48 hours after the application of HFNC. The causes of death in the hypercapnia group were respiratory failure in eight patients, septic shock in one patient, and cardiac arrest in one patient. The eight patients in the hypercapnia group who died because of respiratory failure had an insufficient reduction in CO2 (–2.6±8.5 mm Hg for 48 hours) compared with the other 10 patients (–18.1±11.5 mm Hg for 48 hours, P<0.001).
DISCUSSION
We found a significant decrease in PaCO2 over time after use of an HFNC in patients with acute hypercapnic respiratory failure given O2 therapy via a face mask. The amount of CO2 washout in the hypercapnia group was significantly related to the initial PaCO2 level but not to the respiratory rate or O2 flow rate. Physiological parameters such as pH, PaO2, and respiratory rate improved over time after the use of an HFNC in both groups. The applied O2 flow rate did not differ significantly between the groups during the 48 hours of HFNC use. FiO2 was consistently set higher in the nonhypercapnia group. Inhospital mortality and mean survival time did not differ significantly between the hypercapnia and nonhypercapnia groups.
Our results show that use of an HFNC in the hypercapnia group did not necessarily exacerbate CO2 retention, but instead seemed to be beneficial for CO2 removal, which was not observed in the nonhypercapnia group. This could indicate that the HFNC reduced the PaCO2 level by increasing the clearance of CO2 from anatomical dead spaces. Increased dead space is a well-known mechanism underlying hypercapnia and insufficient ventilation [20]. Rapid shallow breathing, which is commonly observed in acute respiratory failure, can increase the dead space, and increased dead space can contribute to hypercapnia [21]. Therefore, the patients in the hypercapnic group were more likely than those in the nonhypercapnic group to have had large dead-space ventilation. Our data thus suggest that the reduction in PaCO2 in the hypercapnic group occurred through the HFNC “sweeping” CO2 from the dead space.
Recent studies have shown that continuous positive airway pressure (CPAP) is beneficial for inducing CO2 washout. In COPD and COPD overlap syndrome, CPAP can be useful for gas exchange in hypercapnic patients [22,23]. Our findings are consistent with those of a small prospective clinical study that showed that HFNC was more helpful for CO2 reduction than a mask [24]. HFNC is primarily intended to provide a constantly high FiO2, but it also supplies 1.5–3.1 cm H2O of CPAP and reduces airway resistance [25,26]. The effects of HFNC on airway pressure or resistance could be one reason for the reduction in PaCO2 in our study.
It is important to know why the patients in the hypercapnia group were not given NIV or invasive ventilation. Seven patients (or their family) refused to start NIV or invasive ventilation, and 11 patients could not tolerate NIV but could tolerate an HFNC. Even though four patients still exhibited CO2 retention after use of an HFNC, NIV or mechanical ventilation was not applied because they refused that treatment. One patient was intubated after 48 hours. The decision to use an HFNC seemed to be heterogeneous and depended largely on each patient’s preference for or tolerance of the treatment modality.
CO2 retention is caused by ventilatory impairment, which can result from various diseases [11]. Ventilation support with fractionated O2 therapy is the principal therapy used to manage acute hypercapnia [25]. O2 therapy with a high FiO2 aggravates CO2 retention in COPD patients [27]. However, an HFNC can supply a stable flow of O2 with a high FiO2. An HFNC is beneficial for oxygenation, but not ventilation, compared with conventional O2 therapy [28]. Despite some controversy, several clinical trials involving an HFNC in hypercapnic patients have been conducted [15-18]. The background rationale for these trials is the physiological principle that efficient ventilation in the form of an HFNC could reduce dead space [7,8]. An HFNC could, therefore, be a promising alternative or intermediate option before the use of NIV because it has better clinical outcomes in some patients with acute respiratory failure [29]. Our study also shows how physiological parameters improved with time after the change from a face mask to an HFNC, which might have decreased the anatomic dead space. Although four patients in the hypercapnia group became worse with the use of an HFNC, there was sufficient time for them to try NIV again if requested. Given that the PaCO2 changed little with use of an HFNC in patients from the hypercapnia group who died due to respiratory failure, a sufficient reduction in PaCO2 with HFNC use might be a good prognostic indicator.
This study has several limitations. First, it was conducted retrospectively, and unknown confounding factors could not be controlled. However, we performed propensity score matching to minimize the effects of confounding variables. Second, our study population did not represent general patients with acute respiratory failure. Although pneumonia accounted for more than half of the causes of respiratory failure, our patients also had other causative diseases. A considerable number of patients had a terminal status and chose to use an HFNC to avoid invasive procedures or uncomfortable treatments. Therefore, our study suggests that an HFNC might be tried before intubation in patients who cannot tolerate noninvasive positive ventilation, but it is unclear whether this would be beneficial in a specific causative disease. Third, patients who were intubated or noninvasively ventilated within 48 hours of HFNC use were excluded because their serial physiological parameters could have been affected by the use of supported gas ventilation. Fourth, we did not evaluate patients with a severe condition who needed immediate intubation for severe respiratory acidosis, a low level of consciousness, or intractable lung injury. Further studies are needed to identify which subgroups of patients with acute hypercapnic failure can benefit from the use of an HFNC. Finally, we could not confirm whether improvements in physiological parameters were related to better clinical outcomes. We analyzed a single arm from a cohort database in which the patients started HFNC when acute respiratory failure was diagnosed.
In conclusion, HFNC use decreased PaCO2 in patients with various causes of acute hypercapnic respiratory failure. The results of the present study apply to the limited study population who used an HFNC for at least 48 hours.
KEY MESSAGES
▪ After switching from conventional oxygen therapy with facial mask to high-flow nasal cannula, decrease in arterial partial pressure of carbon dioxide (PaCO2), consequent pH normalization, and recovery of respiratory rate were found during 48 hours among patients with acute hypercapnic respiratory failure.
▪ The amount of CO2 washout in the hypercapnia group was significantly related to the initial PaCO2 level but not to the respiratory rate or O2 flow rate.
▪ In propensity score-matched population, in-hospital mortality and mean survival time did not differ significantly between the hypercapnia and nonhypercapnia groups.
NOTES
-
CONFLICT OF INTEREST No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conceptualization: HWL, SML. Data curation & Formal analysis: HWL. Methodology: HWL, SMC, JL, YSP, SML. Project administration: HWL, SML. Visualization: HWL. Writing - original draft: HWL. Writing - review & editing: CHL, CGY, YWK, SKH, SML.
Figure 1.Flowchart showing the classification and propensity score matching of acute respiratory failure patients. HFNC: high-flow nasal cannula.
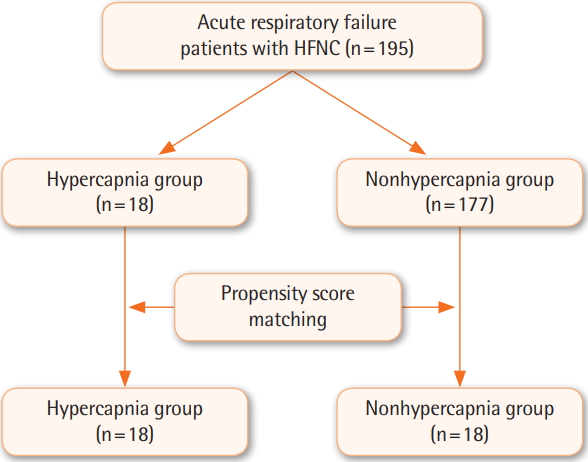
Figure 2.Sequential measurements of arterial partial pressure of carbon dioxide (PaCO2, A), pH (B), and arterial partial pressure of oxygen (PaO2, C) during the use of a high-flow nasal cannula.
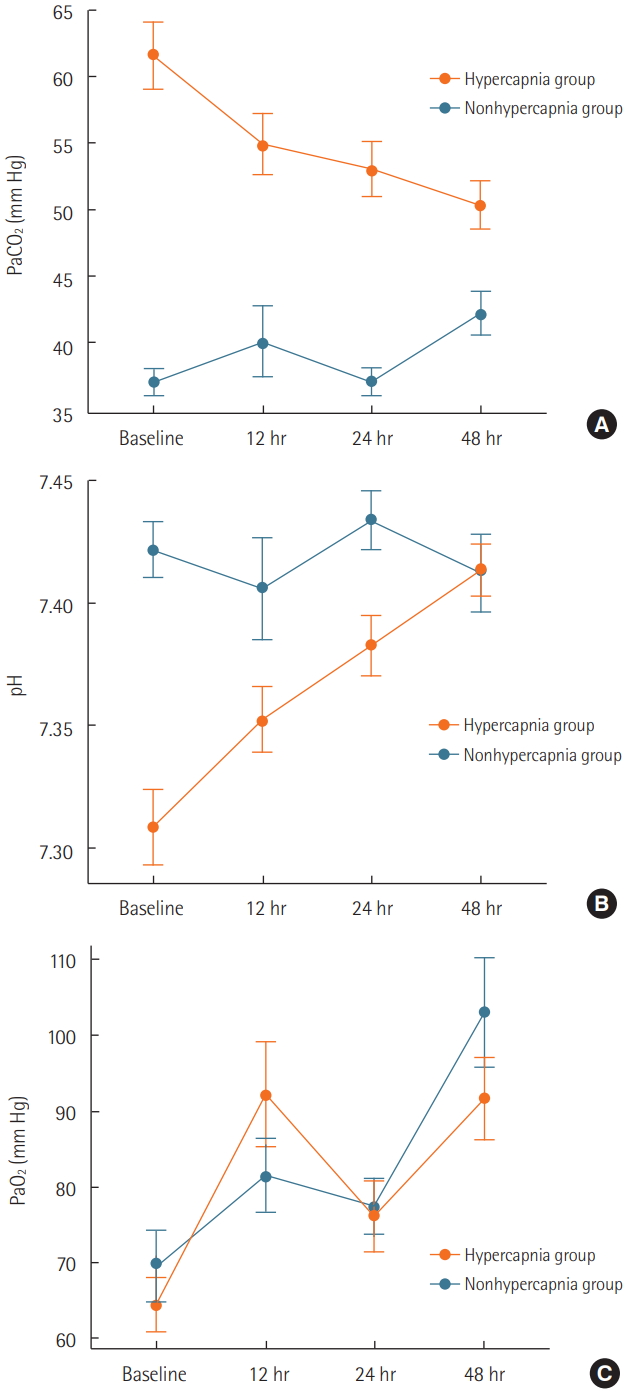
Figure 3.Association between carbon dioxide (CO2) washout during the first 12 hours and initial arterial partial pressure of carbon dioxide (PaCO2) level.
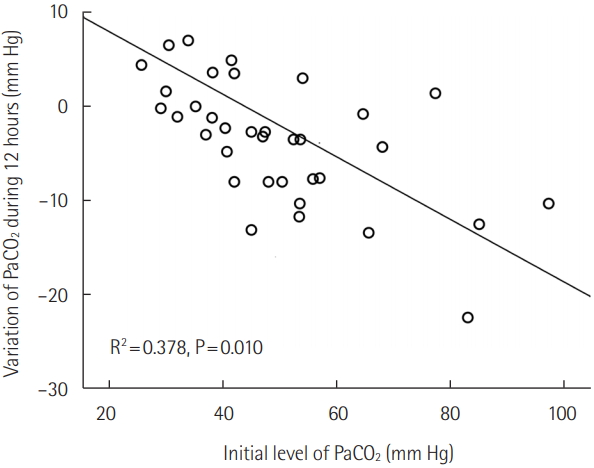
Figure 4.Sequential measurements of respiratory rate (A) and heart rate (B) during the use of a high-flow nasal cannula.
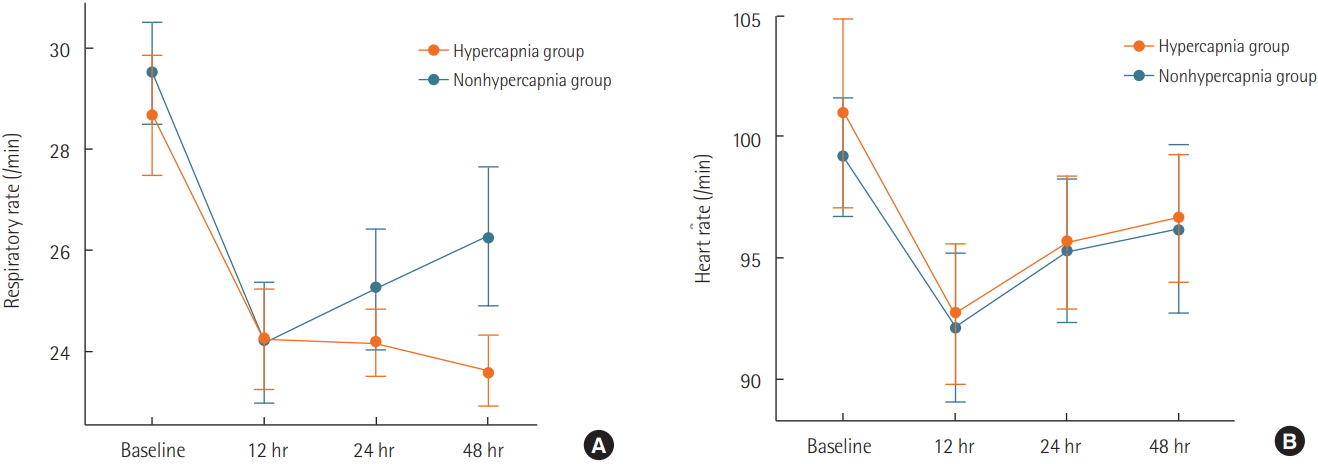
Figure 5.Sequential measurements of fraction of inspired oxygen (FiO2, A) and oxygen (O2) flow rate (B) during the use of a high-flow nasal cannula.
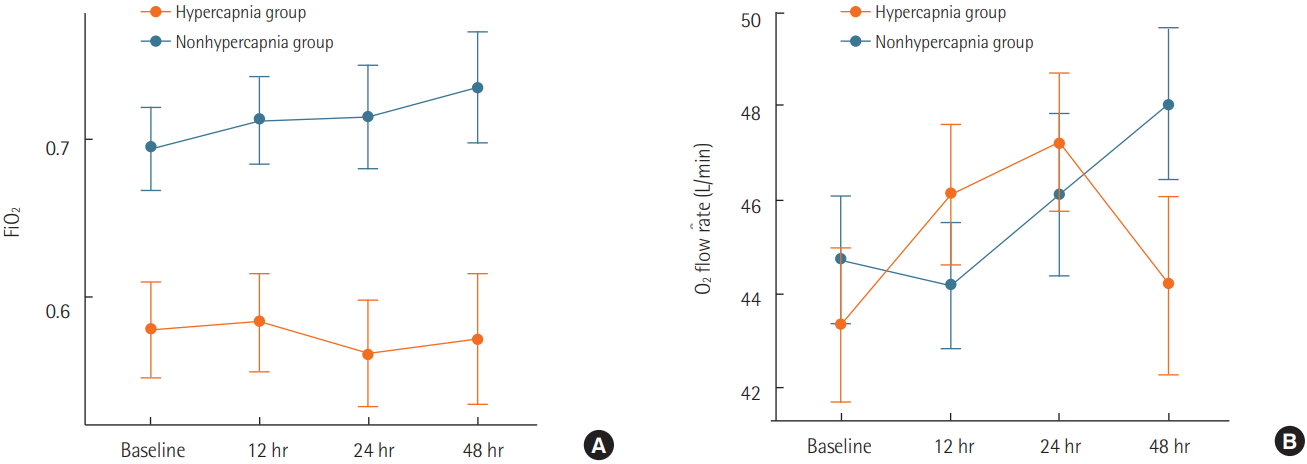
Table 1.Baseline characteristics in the total study population
|
Variable |
Hypercapnia group (n=18) |
Nonhypercapnia group (n=177) |
P-value |
|
Age (yr) |
70.5±12.2 |
66.0±13.1 |
0.166 |
|
Male sex |
16 (88.9) |
116 (65.6) |
0.044 |
|
Body mass index (kg/m2) |
20.9±2.7 |
21.4±3.7 |
0.601 |
|
Glasgow coma scale |
14.5±1.2 |
14.9±0.4 |
0.243 |
|
Do not resuscitate |
11 (61.1) |
95 (53.7) |
0.546 |
|
Do not intubate |
7 (38.9) |
59 (33.3) |
0.635 |
|
Department |
|
|
|
|
Medical intensive care unit |
18 (100) |
166 (93.8) |
0.276 |
|
Previous history of ICU admission |
6 (33.3) |
|
- |
|
Underlying disease |
|
|
|
|
Cardiovascular disease |
8 (44.4) |
34 (19.2) |
0.013 |
|
Cardiomyopathy |
6 (33.3) |
46 (26.0) |
0.502 |
|
Diabetes mellitus |
5 (27.8) |
49 (27.7) |
0.993 |
|
Chronic respiratory disease |
8 (44.4) |
46 (26.0) |
0.095 |
|
Malignancy |
9 (50.0) |
107 (60.5) |
0.389 |
|
Immune deficiency |
6 (33.3) |
109 (61.6) |
0.020 |
|
Liver cirrhosis |
4 (22.2) |
17 (9.6) |
0.100 |
|
Chronic kidney disease |
5 (27.8) |
27 (15.3) |
0.172 |
|
Blood test |
|
|
|
|
Total white blood cell count (/μl) |
16,000±27,034 |
11,682±8,323 |
0.509 |
|
Hematocrit (%) |
32.5±7.0 |
31.4±5.8 |
0.433 |
|
Creatinine (mg/dl) |
2.2±2.1 |
1.4±1.3 |
0.161 |
|
PH |
7.31±0.09 |
7.43±0.07 |
<0.001 |
|
PaO2 (mm Hg) |
64.5±21.4 |
73.0±25.2 |
0.168 |
|
PaCO2 (mm Hg) |
61.5±15.1 |
34.6±5.9 |
<0.001 |
Table 2.Assessment of the clinical conditions in the total population
|
Variable |
Hypercapnia group (n=18) |
Nonhypercapnia group (n=177) |
P-value |
|
Cause of respiratory failurea
|
|
|
|
|
Pneumonia |
11 (61.1) |
121 (68.4) |
0.531 |
|
Disease progressionb
|
3 (16.7) |
21 (11.9) |
0.555 |
|
Pulmonary edema |
6 (33.3) |
31 (17.5) |
0.103 |
|
Acute exacerbation of COPD |
3 (16.7) |
10 (5.6) |
0.074 |
|
Post-extubation respiratory failure |
2 (11.1) |
16 (9.0) |
0.772 |
|
Sepsis |
1 (5.6) |
13 (7.3) |
0.779 |
|
Pulmonary embolism |
0 |
6 (3.4) |
0.428 |
|
Other causes |
1 (5.6) |
8 (4.5) |
0.842 |
|
Initial vital sign |
|
|
|
|
Mean blood pressure (mm Hg) |
91±15 |
92±15.0 |
0.537 |
|
Heart rate (/min) |
101±23 |
103±22 |
0.736 |
|
Respiratory rate (/min) |
29±7 |
27±7 |
0.434 |
|
Body temperature (°C) |
37.4±0.7 |
37.4±0.9 |
0.931 |
|
Oxygen saturation (%) |
90±6 |
90±6 |
0.609 |
|
Use of inotropics |
|
|
|
|
Dobutamine |
0 |
3 (1.7) |
0.567 |
|
Dopamine |
0 |
11 (6.2) |
0.276 |
|
Norepinephrine |
2 (11.1) |
14 (7.9) |
0.699 |
|
Initial setting of high flow oxygen therapy |
|
|
|
|
O2 flow rate (L/min) |
43±10 |
42±9 |
0.555 |
|
FiO2
|
0.58±0.18 |
0.66±0.16 |
0.037 |
|
APACHE II score |
17.8±7.1 |
17.6±6.3 |
0.886 |
|
SOFA score |
6.2±3.1 |
6.5±3.0 |
0.662 |
|
PF ratio |
133±92 |
118±54 |
0.508 |
Table 3.Baseline characteristics in the propensity score-matched population
|
Variable |
Hypercapnia group (n=18) |
Nonhypercapnia group (n=18) |
P-value |
|
Age (yr) |
70.5±12.2 |
72.2±9.3 |
0.648 |
|
Male sex |
16 (88.9) |
17 (94.4) |
0.546 |
|
Body mass index (kg/m2) |
20.9±2.7 |
20.8±2.5 |
0.879 |
|
Glasgow coma scale |
14.5±1.2 |
14.8±0.4 |
0.378 |
|
Do not resuscitate |
11 (61.1) |
10 (55.6) |
0.735 |
|
Do not intubate |
7 (38.9) |
6 (33.3) |
0.729 |
|
Department |
|
|
|
|
Medical ICU |
18 (100) |
18 (100) |
- |
|
Previous history of ICU admission |
6 (33.3) |
6 (33.3) |
1.000 |
|
Underlying disease |
|
|
|
|
Cardiovascular disease |
8 (44.4) |
11 (61.1) |
0.317 |
|
Cardiomyopathy |
6 (33.3) |
8 (44.4) |
0.494 |
|
Diabetes mellitus |
5 (27.8) |
5 (27.8) |
1.000 |
|
Chronic respiratory disease |
8 (44.4) |
11 (61.1) |
0.317 |
|
Malignancy |
9 (50.0) |
6 (33.3) |
0.310 |
|
Immune deficiency |
6 (33.3) |
4 (22.2) |
0.457 |
|
Liver cirrhosis |
4 (22.2) |
3 (16.7) |
0.674 |
|
Chronic kidney disease |
5 (27.8) |
6 (33.3) |
0.717 |
|
Blood test |
|
|
|
|
Total white blood cell count (/μl) |
16,000±27,034 |
16,386±11,984 |
0.956 |
|
Hematocrit (%) |
32.5±7.0 |
33.3±5.8 |
0.721 |
|
Creatinine (mg/dl) |
2.2±2.1 |
2.1±1.5 |
0.878 |
|
pH |
7.31±0.09 |
7.42±0.07 |
<0.001 |
|
PaO2 (mm Hg) |
64.5±21.4 |
69.6±28.1 |
0.542 |
|
PaCO2 (mm Hg) |
61.5±15.1 |
37.1±6.1 |
<0.001 |
Table 4.Assessment of clinical conditions in the propensity score–matched population
|
Variable |
Hypercapnia group (n=18) |
Nonhypercapnia group (n=18) |
P-value |
|
Cause of respiratory failurea
|
|
|
|
|
Pneumonia |
11 (61.1) |
12 (66.7) |
0.729 |
|
Disease progressionb
|
3 (16.7) |
2 (11.1) |
0.630 |
|
Pulmonary edema |
6 (33.3) |
7 (38.9) |
0.729 |
|
Acute exacerbation of COPD |
3 (16.7) |
5 (27.8) |
0.423 |
|
Post-extubation respiratory failure |
2 (11.1) |
2 (11.1) |
1.000 |
|
Sepsis |
1 (5.6) |
1 (5.6) |
1.000 |
|
Pulmonary embolism |
0 |
0 |
- |
|
Other causes |
1 (5.6) |
2 (11.1) |
0.546 |
|
Initial vital sign |
|
|
|
|
Mean blood pressure (mm Hg) |
91±15 |
91±13 |
0.914 |
|
Heart rate (/min) |
101±23 |
99±15 |
0.786 |
|
Respiratory rate (/min) |
29±7 |
30±6 |
0.708 |
|
Body temperature (°C) |
37.4±0.7 |
37.1±0.7 |
0.169 |
|
Oxygen saturation (%) |
90±6 |
90±6 |
0.775 |
|
Use of inotropics |
|
|
|
|
Dobutamine |
0 |
1 (5.6) |
1.000 |
|
Dopamine |
0 |
2 (11.1) |
0.486 |
|
Norepinephrine |
2 (11.1) |
1 (5.6) |
1.000 |
|
Initial setting of high-flow O2 therapy |
|
|
|
|
O2 flow rate (L/min) |
43±10 |
45±8 |
0.648 |
|
FiO2
|
0.58±0.18 |
0.69±0.16 |
0.052 |
|
APACHE II score |
17.8±7.1 |
17.7±4.7 |
0.956 |
|
SOFA score |
6.2±3.1 |
5.8±2.3 |
0.718 |
|
PF ratio |
133±92 |
103±39 |
0.221 |
Table 5.Clinical outcomes in the propensity score-matched population
|
Variable |
Hypercapnia group (n=18) |
Nonhypercapnia group (n=18) |
P-value |
|
All-cause mortality |
10 (55.6) |
11 (61.1) |
0.735 |
|
Cause of death |
|
|
0.867 |
|
Respiratory failure |
8 (80.0) |
8 (72.7) |
|
|
Septic shock |
1 (10.0) |
2 (18.2) |
|
|
Cardiac arrest |
1 (10.0) |
1 (9.1) |
|
|
Others |
|
|
|
|
Survival time during the 28 days after initiation of HFNC (day) |
16.9±9.7 |
17.2±5.4 |
0.522 |
|
Day without HFNC in 7 days |
1.9±1.5 |
2.2±1.8 |
0.687 |
|
Day without HFNC in 14 days |
8.8±1.8 |
8.1±3.7 |
0.462 |
References
- 1. Hernández G, Roca O, Colinas L. High-flow nasal cannula support therapy: new insights and improving performance. Crit Care 2017;21:62. ArticlePubMedPMC
- 2. Curley GF, Laffy JG, Zhang H, Slutsky AS. Noninvasive respiratory support for acute respiratory failure-high flow nasal cannula oxygen or non-invasive ventilation? J Thorac Dis 2015;7:1092-7.PubMedPMC
- 3. Nishimura M. High-flow nasal cannula oxygen therapy in adults. J Intensive Care 2015;3:15. ArticlePubMedPMCPDF
- 4. Dysart K, Miller TL, Wolfson MR, Shaffer TH. Research in high flow therapy: mechanisms of action. Respir Med 2009;103:1400-5.ArticlePubMed
- 5. Sztrymf B, Messika J, Mayot T, Lenglet H, Dreyfuss D, Ricard JD. Impact of high-flow nasal cannula oxygen therapy on intensive care unit patients with acute respiratory failure: a prospective observational study. J Crit Care 2012;27:324-e9-13.Article
- 6. Itagaki T, Okuda N, Tsunano Y, Kohata H, Nakataki E, Onodera M, et al. Effect of high-flow nasal cannula on thoraco-abdominal synchrony in adult critically ill patients. Respir Care 2014;59:70-4.ArticlePubMed
- 7. Möller W, Celik G, Feng S, Bartenstein P, Meyer G, Oliver E, et al. Nasal high flow clears anatomical dead space in upper airway models. J Appl Physiol (1985) 2015;118:1525-32.ArticlePubMedPMC
- 8. Mündel T, Feng S, Tatkov S, Schneider H. Mechanisms of nasal high flow on ventilation during wakefulness and sleep. J Appl Physiol (1985) 2013;114:1058-65.ArticlePubMedPMC
- 9. Corley A, Caruana LR, Barnett AG, Tronstad O, Fraser JF. Oxygen delivery through high-flow nasal cannulae increase endexpiratory lung volume and reduce respiratory rate in postcardiac surgical patients. Br J Anaesth 2011;107:998-1004.ArticlePubMedPDF
- 10. Riera J, Pérez P, Cortés J, Roca O, Masclans JR, Rello J. Effect of high-flow nasal cannula and body position on end-expiratory lung volume: a cohort study using electrical impedance tomography. Respir Care 2013;58:589-96.ArticlePubMed
- 11. Davidson AC, Banham S, Elliott M, Kennedy D, Gelder C, Glossop A, et al. BTS/ICS guideline for the ventilatory management of acute hypercapnic respiratory failure in adults. Thorax 2016;71 Suppl 2:ii1-35.ArticlePubMed
- 12. Diaz O, Iglesia R, Ferrer M, Zavala E, Santos C, Wagner PD, et al. Effects of noninvasive ventilation on pulmonary gas exchange and hemodynamics during acute hypercapnic exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1997;156:1840-5.ArticlePubMed
- 13. Schönhofer B, Sortor-Leger S. Equipment needs for noninvasive mechanical ventilation. Eur Respir J 2002;20:1029-36.ArticlePubMed
- 14. Mehta S, Hill NS. Noninvasive ventilation. Am J Respir Crit Care Med 2001;163:540-77.ArticlePubMed
- 15. Fraser JF, Spooner AJ, Dunster KR, Anstey CM, Corley A. Nasal high flow oxygen therapy in patients with COPD reduces respiratory rate and tissue carbon dioxide while increasing tidal and end-expiratory lung volumes: a randomized crossover trial. Thorax 2016;71:759-61.ArticlePubMedPMC
- 16. Bräunlich J, Köhler M, Wirtz H. Nasal highflow improves ventilation in patients with COPD. Int J Chron Obstruct Pulmon Dis 2016;11:1077-85.ArticlePubMedPMC
- 17. Chatila W, Nugent T, Vance G, Gaughan J, Criner GJ. The effects of high-flow vs low-flow oxygen on exercise in advanced obstructive airways disease. Chest 2004;126:1108-15.ArticlePubMed
- 18. Pilcher J, Eastlake L, Richards M, Power S, Cripps T, Bibby S, et al. Physiological effects of titrated oxygen via nasal highflow cannulae in COPD exacerbations: a randomized controlled cross-over trial. Respirology 2017;22:1149-55.ArticlePubMed
- 19. British Thoracic Society Standards of Care Committee. Noninvasive ventilation in acute respiratory failure. Thorax 2002;57:192-211.ArticlePubMedPMC
- 20. Rawat D, Sharma S. Hypercapnea. Treasure Island: StatPearls Publishing. 2019.
- 21. Jubran A. Rapid shallow breathing: causes and consequences. In: Mancebo J, , Net A, , Brochard L. In: Mechanical ventilation and weaning. Berlin, Heidelberg, Springer Berlin-Heidelberg. 2002, pp 161-8.
- 22. Miro AM, Shivaram U, Hertig I. Continuous positive airway pressure in COPD patients in acute hypercapnic respiratory failure. Chest 1993;103:266-8.ArticlePubMed
- 23. Jaoude P, Kufel T, El-Solh AA. Survival benefit of CPAP favors hypercapnic patients with the overlap syndrome. Lung 2014;192:251-8.ArticlePubMedPDF
- 24. Mauri T, Eronia N, Turrini C, Grasselli G, Bellani G, Pesenti A. High flow nasal cannula improves lung aeration and enhances CO2 removal in hypoxemic critically ill patients. Intensive Care Med Exp 2015;3:A176. ArticlePMC
- 25. Austin MA, Wills KE, Blizzard L, Walters EH, Wood-Baker R. Effect of high flow oxygen on mortality in chronic obstructive pulmonary disease patients in prehospital setting: randomised controlled trial. BMJ 2010;341:c5462. ArticlePubMedPMC
- 26. Chang GY, Cox CA, Shaffer TH. Nasal cannula, CPAP, and highflow nasal cannula: effect of flow on temperature, humidity, pressure, and resistance. Biomed Instrum Technol 2011;45:69-74.ArticlePubMed
- 27. Jeffrey AA, Warren PM, Flenley DC. Acute hypercapnic respiratory failure in patients with chronic obstructive lung disease: risk factors and use of guidelines for management. Thorax 1992;47:34-40.ArticlePubMedPMC
- 28. Lee CC, Mankodi D, Shaharyar S, Ravindranathan S, Danckers M, Herscovici P, et al. High flow nasal cannula versus conventional oxygen therapy and non-invasive ventilation in adults with acute hypoxemic respiratory failure: a systematic review. Respir Med 2016;121:100-8.ArticlePubMed
- 29. Coudroy R, Jamet A, Petua P, Robert R, Frat JP, Thille AW. Highflow nasal cannula oxygen therapy versus noninvasive ventilation in immunocompromised patients with acute respiratory failure: an observational cohort study. Ann Intensive Care 2016;6:45. ArticlePubMedPMCPDF
Citations
Citations to this article as recorded by

- Comparison of preoxygenation with a high-flow nasal cannula and a simple face mask before intubation in patients with head and neck cancer
Jun-Young Jo, Jungpil Yoon, Heeyoon Jang, Wook-Jong Kim, Seungwoo Ku, Seong-Soo Choi
Acute and Critical Care.2024; 39(1): 61. CrossRef - Efficacy and safety of high-flow nasal cannula therapy in elderly patients with acute respiratory failure
J.M. Carratalá, S. Diaz-Lobato, B. Brouzet, P. Más-Serrano, J.L.S. Rocamora, A.G. Castro, A.G. Varela, S.M. Alises
Pulmonology.2023;[Epub] CrossRef - Successful noninvasive ventilation in a severely acidotic and hypercapnic comatose COVID-19 patient with multiple comorbidities: a case report
Joseph Abraham Poonuraparampil, Habib Md Reazaul Karim, Manu P Kesavankutty, Porika Prashanth Nayak
Acute and Critical Care.2022; 37(1): 120. CrossRef - Comparison of Conventional Oxygen Therapy With High-Flow Nasal Oxygenation in the Management of Hypercapnic Respiratory Failure
Jitendra Pratap Singh, Deepak Malviya, Samiksha Parashar, Soumya Sankar Nath, Archana Gautam, Neha Shrivastava
Cureus.2022;[Epub] CrossRef - Current Considerations in Emergency Airway Management
Andrew Pirotte, Vivek Panchananam, Matthew Finley, Austin Petz, Tom Herrmann
Current Emergency and Hospital Medicine Reports.2022; 10(4): 73. CrossRef - S/F and ROX indices in predicting failure of high‐flow nasal cannula in children
Ji Hye Kim, Dong In Suh, June Dong Park
Pediatrics International.2022;[Epub] CrossRef - Nasal High‐flow Oxygen Versus Conventional Oxygen Therapy for Acute Severe Asthma Patients: A Pilot Randomized Controlled Trial
Onlak Ruangsomboon, Chok Limsuwat, Nattakarn Praphruetkit, Apichaya Monsomboon, Tipa Chakorn, Brian C. Hiestand
Academic Emergency Medicine.2021; 28(5): 530. CrossRef - Flow Field Analysis of Adult High-Flow Nasal Cannula Oxygen Therapy
Jingen Xia, Jiaqi Chang, Jixiang Liang, Yixuan Wang, Na Wang, Bo Xiao
Complexity.2021; 2021: 1. CrossRef - Treatment of Severe Acute on Chronic Liver Failure
Aarshi Vipani, Christina C. Lindenmeyer, Vinay Sundaram
Journal of Clinical Gastroenterology.2021; 55(8): 667. CrossRef - Efficacy of High-Flow Nasal Cannula Oxygen Therapy in Patients with Mild Hypercapnia
Lingling Su, Qinyu Zhao, Taotao Liu, Yujun Xu, Weichun Li, Aiping Zhang
Lung.2021; 199(5): 447. CrossRef - High-Flow Nasal Cannula Oxygen Therapy Can Be Effective for Patients in Acute Hypoxemic Respiratory Failure with Hypercapnia: a Retrospective, Propensity Score-Matched Cohort Study
SooHyun Bae, Minkyu Han, Changyoung Kim, Hyeji Lee, Jong-Joon Ahn, Jin Hyoung Kim, Byung Ju Kang
Journal of Korean Medical Science.2020;[Epub] CrossRef - High-flow nasal cannula oxygen therapy as an emerging option for respiratory failure: the present and the future
Lucia Spicuzza, Matteo Schisano
Therapeutic Advances in Chronic Disease.2020; 11: 204062232092010. CrossRef - Impact of High-Flow Nasal Cannula on Arterial Blood Gas Parameters in the Emergency Department
Emre Şancı, Feride Ercan Coşkun, Basak Bayram
Cureus.2020;[Epub] CrossRef

 , Sun Mi Choi
, Sun Mi Choi

 PubReader
PubReader ePub Link
ePub Link Cite
Cite