Articles
- Page Path
- HOME > Acute Crit Care > Volume 33(3); 2018 > Article
- Review Article Deep Learning in the Medical Domain: Predicting Cardiac Arrest Using Deep Learning
-
Youngnam Lee1, Joon-myoung Kwon2
 , Yeha Lee1, Hyunho Park1, Hugh Cho1, Jinsik Park2
, Yeha Lee1, Hyunho Park1, Hugh Cho1, Jinsik Park2 -
Acute and Critical Care 2018;33(3):117-120.
DOI: https://doi.org/10.4266/acc.2018.00290
Published online: August 31, 2018
1VUNO, Seoul, Korea
2Department of Emergency Medicine, Mediplex Sejong Hospital, Incheon, Korea
- Corresponding author Joon-myoung Kwon Department of Emergency Medicine, Mediplex Sejong Hospital, 20 Gyeyangmunhwa-ro, Gyeyang-gu, Incheon 21080, Korea Tel: +82-32-240-8000 Fax: +82-32-240-8999 E-mail: kwonjm@sejongh.co.kr
- *The first two authors contributed equally to this study.
Copyright © 2018 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
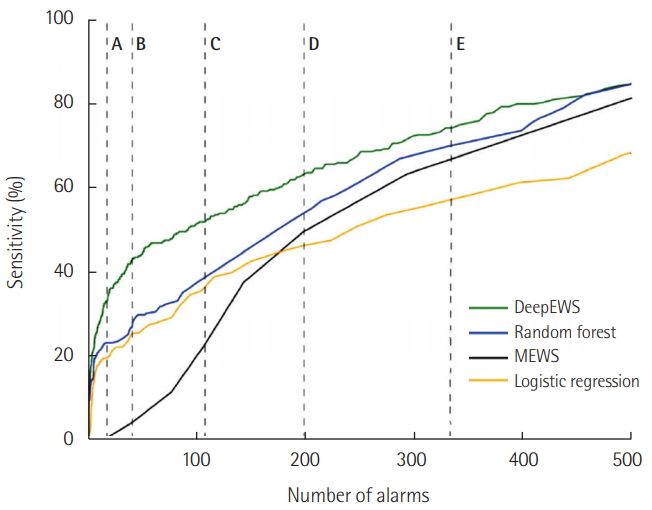
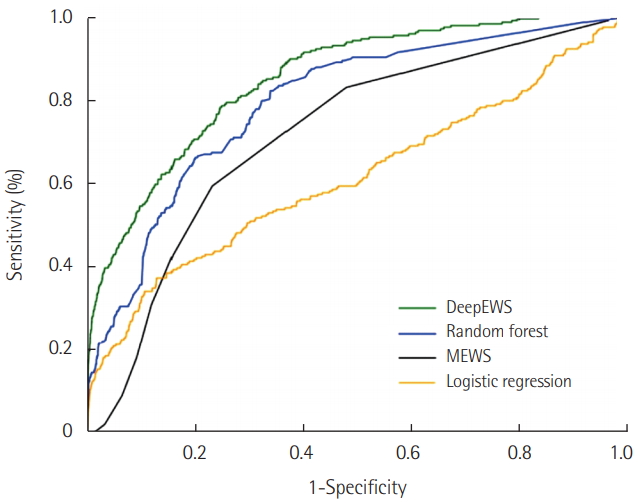
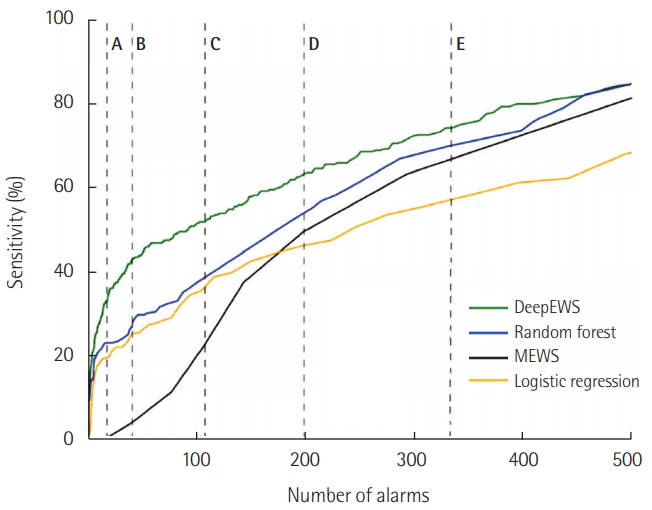
- With the wider adoption of electronic health records, the rapid response team initially believed that mortalities could be significantly reduced but due to low accuracy and false alarms, the healthcare system is currently fraught with many challenges. Rule-based methods (e.g., Modified Early Warning Score) and machine learning (e.g., random forest) were proposed as a solution but not effective. In this article, we introduce the DeepEWS (Deep learning based Early Warning Score), which is based on a novel deep learning algorithm. Relative to the standard of care and current solutions in the marketplace, there is high accuracy, and in the clinical setting even when we consider the number of alarms, the accuracy levels are superior.
INTRODUCTION
MACHINE AND DEEP LEARNING
DEEP LEARNING BASED EARLY WARNING SCORE
CONCLUSION
KEY MESSAGES
-
Youngnam Lee, Joon-myoung Kwon, Yeha Lee, and Jinsik Park were involved in developing DEWS (Deep learning based Early Warning Score). VUNO provided support in the form of salaries for authors (Youngnam Lee, Yeha Lee, Hyunho Park, and Hugh Cho), but did not provide funding and did not have any additional role. No other conflict of interest relevant to this article was reported.
NOTES

- 1. Hillman K, Chen J, Cretikos M, Bellomo R, Brown D, Doig G, et al. Introduction of the medical emergency team (MET) system: a cluster-randomised controlled trial. Lancet 2005;365:2091-7.ArticlePubMed
- 2. Trinkle RM, Flabouris A. Documenting rapid response system afferent limb failure and associated patient outcomes. Resuscitation 2011;82:810-4.ArticlePubMed
- 3. Churpek MM, Yuen TC, Winslow C, Meltzer DO, Kattan MW, Edelson DP. Multicenter comparison of machine learning methods and conventional regression for predicting clinical deterioration on the wards. Crit Care Med 2016;44:368-74.ArticlePubMedPMC
- 4. Gao H, McDonnell A, Harrison DA, Moore T, Adam S, Daly K, et al. Systematic review and evaluation of physiological track and trigger warning systems for identifying at-risk patients on the ward. Intensive Care Med 2007;33:667-79.ArticlePubMed
- 5. Bell MB, Konrad D, Granath F, Ekbom A, Martling CR. Prevalence and sensitivity of MET-criteria in a Scandinavian University Hospital. Resuscitation 2006;70:66-73.ArticlePubMed
- 6. Kwon JM, Lee Y, Lee Y, Lee S, Park J. An algorithm based on deep learning for predicting in-hospital cardiac arrest. J Am Heart Assoc 2018;7:e008678. ArticlePubMedPMC
- 7. Deo RC. Machine learning in medicine. Circulation 2015;132:1920-30.ArticlePubMedPMC
- 8. Gulshan V, Peng L, Coram M, Stumpe MC, Wu D, Narayanaswamy A, et al. Development and validation of a deep learning algorithm for detection of diabetic retinopathy in retinal fundus photographs. JAMA 2016;316:2402-10.ArticlePubMed
- 9. Jha S, Topol EJ. Adapting to artificial intelligence: radiologists and pathologists as information specialists. JAMA 2016;316:2353-4.ArticlePubMed
- 10. LeCun Y, Bengio Y, Hinton G. Deep learning. Nature 2015;521:436-44.ArticlePubMedPDF
References
Figure & Data
References
Citations
- External Validation of Deep Learning-Based Cardiac Arrest Risk Management System for Predicting In-Hospital Cardiac Arrest in Patients Admitted to General Wards Based on Rapid Response System Operating and Nonoperating Periods: A Single-Center Study
Kyung-Jae Cho, Kwan Hyung Kim, Jaewoo Choi, Dongjoon Yoo, Jeongmin Kim
Critical Care Medicine.2024; 52(3): e110. CrossRef - Evaluation of optimal scene time interval for out-of-hospital cardiac arrest using a deep neural network
Seung Jae Shin, Hee Sun Bae, Hyung Jun Moon, Gi Woon Kim, Young Soon Cho, Dong Wook Lee, Dong Kil Jeong, Hyun Joon Kim, Hyun Jung Lee
The American Journal of Emergency Medicine.2023; 63: 29. CrossRef - Short-term load forecasting based on CEEMDAN and Transformer
Peng Ran, Kun Dong, Xu Liu, Jing Wang
Electric Power Systems Research.2023; 214: 108885. CrossRef - Artificial Intelligence in Resuscitation: A Scoping Review
Dmitriy Viderman, Yerkin Abdildin, Kamila Batkuldinova, Rafael Badenes, Federico Bilotta
Journal of Clinical Medicine.2023; 12(6): 2254. CrossRef - Prediction of Out-of-Hospital Cardiac Arrest Survival Outcomes Using a Hybrid Agnostic Explanation TabNet Model
Hung Viet Nguyen, Haewon Byeon
Mathematics.2023; 11(9): 2030. CrossRef - Enhancing breast cancer diagnosis with deep learning and evolutionary algorithms: A comparison of approaches using different thermographic imaging treatments
Alberto Nogales, Fernando Pérez-Lara, Álvaro J. García-Tejedor
Multimedia Tools and Applications.2023; 83(14): 42955. CrossRef - Machine learning pre-hospital real-time cardiac arrest outcome prediction (PReCAP) using time-adaptive cohort model based on the Pan-Asian Resuscitation Outcome Study
Hansol Chang, Ji Woong Kim, Weon Jung, Sejin Heo, Se Uk Lee, Taerim Kim, Sung Yeon Hwang, Sang Do Shin, Won Chul Cha, Marcus Ong
Scientific Reports.2023;[Epub] CrossRef - Attempting cardiac arrest prediction using artificial intelligence on vital signs from Electronic Health Records
Bassel Soudan, Fetna F. Dandachi, Ali Bou Nassif
Smart Health.2022; 25: 100294. CrossRef - BERT Learns From Electroencephalograms About Parkinson’s Disease: Transformer-Based Models for Aid Diagnosis
Alberto Nogales, Alvaro J. Garcia-Tejedor, Ana M. Maitin, Antonio Perez-Morales, Maria Dolores Del Castillo, Juan Pablo Romero
IEEE Access.2022; 10: 101672. CrossRef - Artificial intelligence decision points in an emergency department
Hansol Chang, Won Chul Cha
Clinical and Experimental Emergency Medicine.2022; 9(3): 165. CrossRef - Development of Prediction Models for Acute Myocardial Infarction at Prehospital Stage with Machine Learning Based on a Nationwide Database
Arom Choi, Min Joung Kim, Ji Min Sung, Sunhee Kim, Jayoung Lee, Heejung Hyun, Hyeon Chang Kim, Ji Hoon Kim, Hyuk-Jae Chang
Journal of Cardiovascular Development and Disease.2022; 9(12): 430. CrossRef - Short-Term Load Forecasting Based on Ceemdan and Transformer
Peng Ran, Kun Dong, Xu Liu, Jing Wang
SSRN Electronic Journal .2022;[Epub] CrossRef - A survey of deep learning models in medical therapeutic areas
Alberto Nogales, Álvaro J. García-Tejedor, Diana Monge, Juan Serrano Vara, Cristina Antón
Artificial Intelligence in Medicine.2021; 112: 102020. CrossRef - A predictive framework in healthcare: Case study on cardiac arrest prediction
Samaneh Layeghian Javan, Mohammad Mehdi Sepehri
Artificial Intelligence in Medicine.2021; 117: 102099. CrossRef - Development of Prediction Models for Acute Myocardial Infarction at Prehospital Stage with Machine Learning Based on a Nationwide Database (Preprint)
Arom Choi, Min Joung Kim, Ji Min Sung, Sunhee Kim, Jayong Lee, Heejung Hyun, Ji Hoon Kim, Hyuk-Jae Chang
JMIR Medical Informatics.2021;[Epub] CrossRef - Predicting in-hospital mortality in adult non-traumatic emergency department patients: a retrospective comparison of the Modified Early Warning Score (MEWS) and machine learning approach
Kuan-Han Wu, Fu-Jen Cheng, Hsiang-Ling Tai, Jui-Cheng Wang, Yii-Ting Huang, Chih-Min Su, Yun-Nan Chang
PeerJ.2021; 9: e11988. CrossRef - Cardioinformatics: the nexus of bioinformatics and precision cardiology
Bohdan B Khomtchouk, Diem-Trang Tran, Kasra A Vand, Matthew Might, Or Gozani, Themistocles L Assimes
Briefings in Bioinformatics.2020; 21(6): 2031. CrossRef - Development of a Real-Time Risk Prediction Model for In-Hospital Cardiac Arrest in Critically Ill Patients Using Deep Learning: Retrospective Study
Junetae Kim, Yu Rang Park, Jeong Hoon Lee, Jae-Ho Lee, Young-Hak Kim, Jin Won Huh
JMIR Medical Informatics.2020; 8(3): e16349. CrossRef - Rapid response systems in Korea
Bo Young Lee, Sang-Bum Hong
Acute and Critical Care.2019; 34(2): 108. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite