Perfusion parameters during cardiopulmonary bypass as a predictor of acute kidney injury after aortic valve replacement
Article information

Abstract
Background
Acute kidney injury (AKI) is a major complication after cardiac surgery and significantly affects postoperative mortality and morbidity. This study was conducted to evaluate the association between target pump flow to achieve adequate oxygen delivery (DO2) and postoperative renal function after aortic valve replacement.
Methods
From January 2017 to May 2020, 281 patients (male:female, 160:121; mean age, 68±11 years) who underwent aortic valve replacement were retrospectively reviewed. Target pump flow was calculated based on DO2 level of 280 mL/min/m2. The primary endpoint was postoperative renal dysfunction, defined as the ratio of postoperative peak creatinine level to preoperative value. The ratio of the lowest actual pump flow to the ideal target pump flow, other hemodynamic variables related with cardiopulmonary bypass, intraoperative transfusion, and preoperative characteristics were analyzed to identify factors associated with the primary endpoint using a multivariable linear regression model.
Results
Preoperative and peak postoperative creatinine levels were 0.94±0.33 mg/dl and 1.15±0.56 mg/dl, respectively (ratio, 1.22±0.33). The ideal target pump flow was 4.70±0.59 L/min, whereas the lowest actual pump flow was 3.77±0.47 L/min (ratio, 0.81±0.13). The multivariable model showed that the ratio of the lowest pump flow to target pump flow (β±standard error, –0.405±0.162, P=0.013), as well as sex, stroke history, emergency operation, and transfusion of red blood cells were associated with the primary endpoint.
Conclusions
Low actual nadir pump flow compared to the ideal target pump flow based on DO2 is associated with the risk of AKI after aortic valve replacement.
INTRODUCTION
Acute kidney injury (AKI) is a common postoperative complication that occurs in 20% to 40% of cardiac surgical patients [1-3]. Postoperative AKI is associated with mortality after surgery, which increases up to 50% when renal replacement therapy is required [4]. In addition, even small decreases in glomerular filtration rates might be associated with increased postoperative mortality [5]. Previous studies demonstrated various risk factors associated with occurrence of AKI after cardiac surgery [3,6-8]. These include age, diabetes mellitus, pre-existing renal dysfunction, prolonged cardiopulmonary bypass (CPB) time, and use of adrenergic medications [3,6-8].
In addition to well-known risk factors, recent studies [9-11] have demonstrated that nadir oxygen delivery (DO2) during CPB is the best predictor of AKI after cardiac surgery. These observations have led to the concept of goal-directed perfusion, which is intended to maintain the DO2 level above the critical value during CPB. CPB flow is one of the modifiable risk factors for AKI and has conventionally been largely based on monitoring of a formula based on the cardiac index multiplied by the body surface area of the patient. However, pump flow based solely on a cardiac index does not ensure satisfactory DO2 to the tissues, which can lead to metabolic acidosis, hyperlactatemia, and end-organ ischemia. However, high-level evidence of the association of goal-directed perfusion strategy and postoperative AKI remains lacking. Therefore, this study was conducted to evaluate the association between perfusion parameters during CPB and postoperative renal dysfunction after aortic valve replacement (AVR).
MATERIALS AND METHODS
Patient Characteristics
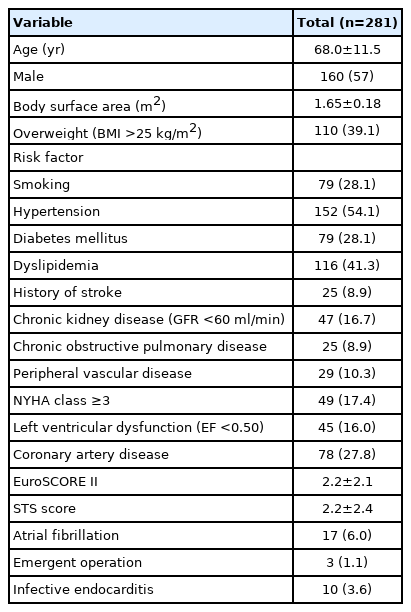
The study protocol was reviewed by the Institutional Review Board of Seoul National University Hospital and approved as a minimal risk retrospective study (IRB No. H-2009-158-1159) that did not require individual consent based on the institutional guidelines for waiving consent. A total of 434 patients who underwent AVR between January 2017 and May 2020, at our institution was retrospectively screened. Patients who underwent concomitant valve surgery other than AVR (n = 40), aortic surgery under total circulatory arrest (n = 68), arrhythmia surgery (n = 32), and those with preoperative end-stage renal disease on dialysis (n = 21) were excluded. A final total of 281 patients was enrolled in the present study. The mean age at operation was 68 ± 11 years, and 160 patients (56.9%) were male. The European System for Cardiac Operative Risk Evaluation (EuroSCORE) II and Society of Thoracic Surgeons (STS) score were 2.2 ±2.1 and 2.2 ±2.4, respectively. Hypertension (n=152, 54.1%), dyslipidemia (n=116, 41.3%), diabetes (n=79, 28.1%), and coronary artery disease (n =78, 27.8%) were the most common comorbidities (Table 1).
Characteristics of the study patients
Surgical Procedures
All operations were performed through median sternotomy and aorto-bicaval cannulation under moderate hypothermia (30°C–32°C). Concomitant procedures comprised coronary artery bypass grafting (n = 35) and closure of patent foramen ovale (n = 12). The mean CPB and aortic cross-clamp times were 147.4±51.6 and 92.2±32.2 minutes, respectively (Table 2).

Operative data of the study patients
Evaluation of Clinical Outcomes
The target pump flow was calculated based on DO2 level of 280 ml/min/m2 and the following equation: DO2= pump flow × (Hb concentration × Hb saturation × 1.36)+(0.003 × PaO2), where Hb, hemoglobin; PaO2, arterial oxygen pressure [12]. Early mortality was defined as any death within 30 days or during the same hospitalization. Postoperative atrial fibrillation was defined as a new onset or any short run of atrial fibrillation. Low cardiac output syndrome (LCOS) was defined as a cardiac index < 2.0 L/min/m2 or a systolic arterial pressure < 90 mm Hg for which the patient required mechanical assistance or high inotropic support such as dopamine or dobutamine in quantities > 5 μg/kg/min. Postoperative respiratory complications included pneumonia or prolonged ventilator support for more than 48 hours.
Statistical Analysis
The primary endpoint was postoperative renal dysfunction, defined as the ratio of the postoperative peak creatinine level to the preoperative value. The statistical analyses were performed using IBM SPSS ver. 23.0 (IBM Corp., Armonk, NY, USA). Continuous and dichotomous variables are expressed as the mean ± standard deviation or median with interquartile range (IQR) and the number with the proportion, respectively. A paired t-test was performed to compare differences between preoperative creatinine levels and postoperative peak creatinine levels.
The ratio of the actual pump flow to the target pump flow based on the DO2 and the presence of other perfusion parameters during CPB such as lowest temperature, mean arterial pressure, hematocrit levels, PaO2, intraoperative red blood cells (RBCs) transfusion, and preoperative characteristics were analyzed to identify factors associated with the primary endpoint. Univariate and multivariable analyses were performed using linear regression models. Variables with a P-value < 0.05 in univariate analyses were entered into a multivariable model. Multi-collinearity was controlled using backward stepwise selection. The results of the multivariable analysis are expressed as P-value, beta coefficient (β), and standard error (SE). A Pvalue < 0.05 was considered statistically significant.
RESULTS
Early Clinical Outcomes
The early mortality rate was 2.5% (7 of 281 patients). Postoperative complications included respiratory complications (n = 24, 8.6%), LCOS (n = 12, 4.3%), stroke (n = 5, 1.8%), and bleeding reoperation (n = 3, 1.1%) (Table 3).

Early clinical outcomes
CPB Variables
The lowest temperature and the lowest mean arterial pressure during CPB were 30.4°C ± 2.4°C and 58.9 ± 8.8 mm Hg, respectively. The lowest hematocrit level was 21.5% ± 3.0%, and the median number of RBCs transfused during CPB was 0.5 (IQR, 0–1.0). Mean PaO2 was 338.4 ± 45.0 mm Hg. Based on the assumed target DO2 index of 280 ml/min/m2, the ideal target pump flow was 4.7 ± 0.6 L/min, and the lowest actual pump flow was 3.8 ± 0.5 L/min during CPB. The ratio of the lowest actual pump flow to the ideal target pump flow was 0.81 ± 0.13 (Table 4).

Cardiopulmonary bypass variables
Changes in Creatinine Level after Surgery
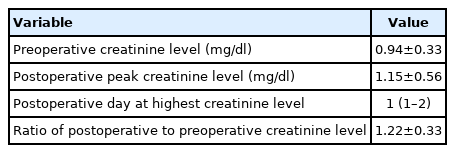
Creatinine increased from a preoperative level of 0.94 ± 0.33 mg/dl to a postoperative peak level of 1.15±0.56 mg/dl (P<0.001). The postoperative creatinine level was highest at postoperative day 1 (IQR, 1–2). The ratio of postoperative peak creatinine level to preoperative creatinine level was 1.22 ± 0.33 (Table 5).
Changes in renal function
Risk Factor Analyses for the Primary Endpoint
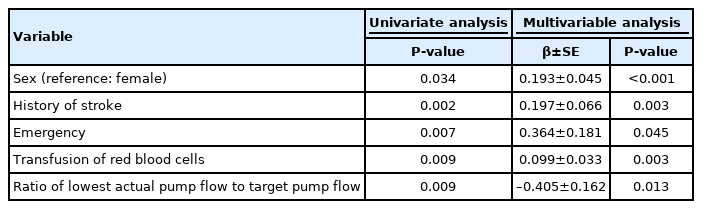
Univariate analyses demonstrated that the ratio of the actual pump flow to the ideal target pump flow (P = 0.009), age, sex, stroke history, EuroScore II, emergency status, hematocrit level, and RBC transfusion during CPB were significant factors associated with the primary endpoint. In the multivariable model, the ratio of the lowest pump flow to the maximum target pump flow (β± SE, –0.405 ± 0.162; P = 0.013), sex (reference: female; 0.193 ± 0.045, P < 0.001), stroke history (0.197 ± 0.066, P = 0.003), emergency (0.364 ± 0.181, P = 0.045), and RBC transfusion (0.099 ± 0.033, P = 0.003) were associated with the primary endpoint for postoperative renal dysfunction (Table 6).
Risk factor analysis for changes in creatinine level after surgery
DISCUSSION
The present study demonstrates that the actual lowest pump flow compared to the target pump flow based on the DO2 is associated with the risk of AKI after AVR. AKI is a well-recognized and clinically significant complication following cardiac surgery under CPB. The range of AKI has been reported to range from 20% to 40% of all cardiac surgical patients depending on the definition used [1-4,13,14]. Even minimal changes in postoperative creatinine values can result in both early and late morbidity and mortality after cardiac surgery [5,15-17]. Several studies have shown that AKI can exponentially increase the postoperative mortality rate to 50% in patients requiring dialysis, compared to that of 0.6% to 2% in patients with no AKI [4,18,19]. Therefore, prevention of this postoperative complication is of paramount importance.
Many studies have discovered independent risk factors leading to renal impairment after cardiac surgery [4,20-30]. However, most of the factors such as age, preoperative comorbidities, and complex surgical procedures are unmodifiable. The present study was designed to determine risk factors that could be modifiable, particularly CPB parameters. Since the incidence of AKI might vary according to type of cardiac operation [2,21,23], only patients who underwent AVR with or without coronary artery bypass graft surgery were enrolled.
Regarding CPB management, the most commonly used bypass flow rates during CPB ranged from 2.2 to 2.5 L/min/m2 [31,32], and it has been suggested that systemic flow rates influence the perfusion of organs other than the brain. A previous prospective observational study [33] showed that low flow on CPB is the major cause of both adverse renal and neurologic outcomes. However, the optimal flow rate that supports the most favorable organ perfusion has yet to be determined, and institutional practices have been largely based on their own experiences. Recently, DO2 has been suggested as an important modifiable parameter that prevents postoperative AKI. Two important variables for perfusion, i.e., hematocrit values and CPB pump flow rates, are incorporated into a single calculation of DO2. A previous study [9], in a retrospective series, found a “critical” DO2 threshold of 272 mL/min/m2. When DO2 level falls below the critical value of 260–270 mL/min/m2, organ deoxygenation can be triggered with subsequent tissue acidosis, causing impaired postoperative renal function. Another study [11] investigated the role of potentially modifiable factors related to CPB management in determining postoperative AKI. The study results demonstrated that low DO2 level during CPB is independently associated with postoperative AKI. They found that a nadir DO2 less than 262 mL/min/m2 was independently associated with development of postoperative AKI.
In the present study, based on the assumed target DO2 level of 280 mL/min/m2, the ideal target pump flow was assumed to be 4.7 ± 0.6 L/min during CPB. Among the various CPB parameters, not the absolute value but the ratio of the nadir pump flow to the ideal target flow based on the DO2 was associated with risk of AKI. In addition, the multivariable model demonstrated that not the nadir hematocrit level during CPB but transfusion was associated with AKI. The relationship between transfusion of RBCs and AKI development has long been reported in surgical literature [2,34]. However, the need for blood transfusion might be just an indicator of increased blood loss and a hypotensive or ischemic state, which is a main pathogenic mechanism of AKI. Therefore, further study is needed to clarify the impact of low hematocrit levels vs. RBC transfusion on clinical outcomes after cardiac surgery.
The present study has limitations that should be recognized. First, this was a retrospective observational study performed in a single institution. Therefore, our models must be validated at multiple centers for broader applicability. Second, the effects of unknown or unmeasured confounders associated with postoperative AKI cannot be ruled out. Finally, the number of enrolled patients in this study was relatively small. In conclusion, low actual nadir pump flow during CPB compared to the ideal target pump flow based on the DO2 is associated with risk of AKI after AVR.
KEY MESSAGES
■ The actual lowest pump flow compared to the target pump flow based on oxygen delivery (DO2) might be a predictor of postoperative acute kidney injury after cardiac surgery.
■ Female sex, stroke history, emergency operation, and transfusion of red blood cells were significant risk factors of postoperative acute kidney injury after cardiac surgery.
Notes
CONFLICT OF INTEREST No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: SHK, HYH. Data curation: SHK, HYH. Formal analysis: SHK, HYH. Methodology: SHK, HYH. Project administration: HYH, SHS, JWC, KHK. Visualization: SHK, HYH. Writing–original draft: YL, SHK, HYH. Writing–review & editing: all authors.