Articles
- Page Path
- HOME > Acute Crit Care > Volume 37(2); 2022 > Article
-
Case Report
Cardiology Acute perimyocarditis mimicking acute myocardial infarction in a 12-year-old boy with duchenne muscular dystrophy -
Ho Jung Choi
 , Hye Won Kwon, Kyung Jin Oh, Mi Kyoung Song
, Hye Won Kwon, Kyung Jin Oh, Mi Kyoung Song -
Acute and Critical Care 2021;37(2):258-262.
DOI: https://doi.org/10.4266/acc.2021.00290
Published online: November 16, 2021
Department of Pediatrics, Seoul National University Hospital, Seoul, Korea
- Corresponding author: Hye Won Kwon Department of Thoracic and Cardiovascular Surgery, Seoul National University Hospital, 101 Daehak-ro, Jongno-gu, Seoul 03080, Korea Tel: +82-2-2072-4306, Fax: +82-2-747-2471, E-mail: drhwkwon@gmail.com
- *Current affiliationHye Won Kwon: Department of Thoracic and Cardiovascular Surgery, Seoul National University Hospital, Seoul, KoreaKyung Jin Oh: Department of Pediatrics, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul, Korea
• Received: March 8, 2021 • Revised: April 30, 2021 • Accepted: April 30, 2021
Copyright © 2022 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
- Differential diagnosis of chest pain in the pediatric population is important but can be challenging. A 12-year-old boy with Duchenne muscular dystrophy presented with chest pain, cardiac enzyme elevation, and convex ST elevations in the inferior leads with reciprocal ST depression in the anterior leads on electrocardiogram. Echocardiography on admission revealed normal left ventricular function. Suspecting acute myocardial infarction, we performed invasive coronary angiography, which revealed normal coronary arteries. A follow-up electrocardiogram showed an acute pericarditis pattern with concave ST elevations in most leads and PR depression, and follow-up echocardiography revealed global left ventricular dysfunction, suggestive of acute perimyocarditis. Ibuprofen was administered for acute pericarditis, and a continuous milrinone infusion was commenced for myocardial dysfunction. The chest pain improved by the next day, and the ST segment elevations normalized on day 4. Echocardiography on day 9 revealed improved left ventricular function. The patient was discharged on day 11, and he is doing well without chest pain through 12 months of follow-up. The last electrocardiogram showed normal sinus rhythm without ST change. Differential diagnosis of acute myocardial infarction and acute perimyocarditis is important for proper treatment strategies and the different prognoses of these two conditions.
CASE REPORT
DISCUSSION
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conceptualization: HWK. Data curation: HJC, KJO. Project administration: HWK. Writing–original draft: HJC. Writing–review & editing: HWK, MKS.
NOTES
SUPPLEMENTARY MATERIALS
Supplementary Video 2.
Figure 1.(A) Initial chest radiograph showing no cardiothoracic abnormalities. (B) Echocardiography performed on the second day of hospitalization showing mild global left ventricular dysfunction (ejection fraction, 41%) without regional wall motion abnormalities. (C, D) Cardiac magnetic resonance imaging showing late gadolinium enhancement (arrowheads) in the subepicardium of the left ventricular inferolateral and mid-septal walls.

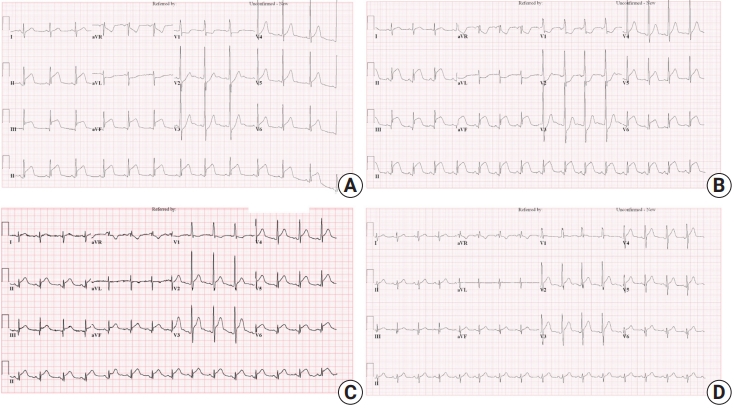
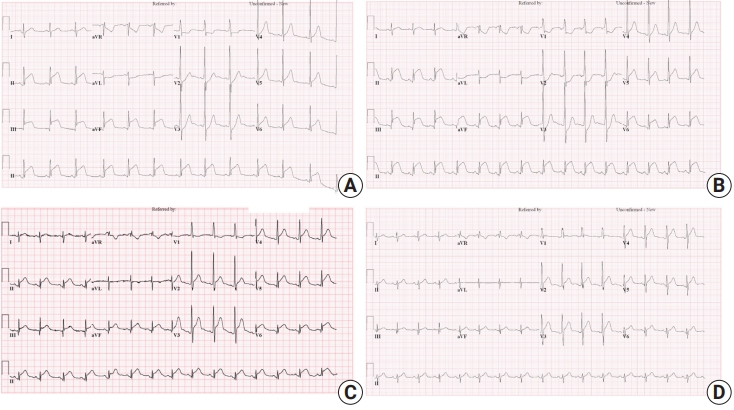
Figure 2.(A) Initial electrocardiogram showing ST elevations in the inferior leads and reciprocal ST depressions in the anterior leads. (B) Electrocardiogram, 3 hours post-admission, showing aggravated convex ST elevations and reciprocal changes. (C) Electrocardiogram, 12 hours post-admission, showing concave ST elevations in most leads and PR depression. (D) ST segment elevations normalized on the 4th day of hospitalization after ibuprofen treatment. aVR: lead augmented vector right; aVL: lead augmented vector left; aVF: lead augmented vector foot.
- 1. de Bliek EC. ST elevation: differential diagnosis and caveats. A comprehensive review to help distinguish ST elevation myocardial infarction from nonischemic etiologies of ST elevation. Turk J Emerg Med 2018;18:1-10.ArticlePubMedPMC
- 2. Deshpande A, Birnbaum Y. ST-segment elevation: distinguishing ST elevation myocardial infarction from ST elevation secondary to nonischemic etiologies. World J Cardiol 2014;6:1067-79.ArticlePubMedPMC
- 3. Adler Y, Charron P, Imazio M, Badano L, Barón-Esquivias G, Bogaert J, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2015;36:2921-64.PubMed
- 4. Kindermann I, Barth C, Mahfoud F, Ukena C, Lenski M, Yilmaz A, et al. Update on myocarditis. J Am Coll Cardiol 2012;59:779-92.ArticlePubMed
- 5. Cooper LT, Baughman KL, Feldman AM, Frustaci A, Jessup M, Kuhl U, et al. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology Endorsed by the Heart Failure Society of America and the Heart Failure Association of the European Society of Cardiology. Eur Heart J 2007;28:3076-93.ArticlePubMed
- 6. Bozkurt B, Colvin M, Cook J, Cooper LT, Deswal A, Fonarow GC, et al. Current diagnostic and treatment strategies for specific dilated cardiomyopathies: a scientific statement from the American Heart Association. Circulation 2016;134:e579-646.ArticlePubMed
- 7. Sagar S, Liu PP, Cooper LT Jr. Myocarditis. Lancet 2012;379:738-47.ArticlePubMed
- 8. Liu PP, Mason JW. Advances in the understanding of myocarditis. Circulation 2001;104:1076-82.ArticlePubMed
- 9. Nigro G, Comi LI, Politano L, Bain RJ. The incidence and evolution of cardiomyopathy in Duchenne muscular dystrophy. Int J Cardiol 1990;26:271-7.ArticlePubMed
- 10. Verhaert D, Richards K, Rafael-Fortney JA, Raman SV. Cardiac involvement in patients with muscular dystrophies: magnetic resonance imaging phenotype and genotypic considerations. Circ Cardiovasc Imaging 2011;4:67-76.PubMedPMC
References
Figure & Data
References
Citations
Citations to this article as recorded by 
- Pediatric Chest Pain: A Review of Diagnostic Tools in the Pediatric Emergency Department
Szu-Wei Huang, Ying-Kuo Liu
Diagnostics.2024; 14(5): 526. CrossRef - Successful treatment of acute myocardial injury of Duchenne muscular dystrophy with steroids: a case report
Merve Oğuz, Dolunay Gürses, Furkan Ufuk, Münevver Yılmaz, Olcay Güngör
Journal of Cardiothoracic Surgery.2023;[Epub] CrossRef - Comprehensive cardiac magnetic resonance T1, T2, and extracellular volume mapping to define Duchenne cardiomyopathy
Sudeep D. Sunthankar, Kristen George-Durrett, Kimberly Crum, James C. Slaughter, Jennifer Kasten, Frank J. Raucci, Larry W. Markham, Jonathan H. Soslow
Journal of Cardiovascular Magnetic Resonance.2023; 25(1): 44. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite