Incidence and associated factors of pediatric post-intensive care syndrome using the VSCAREMD model
Article information

Abstract
Background
The VSCAREMD model is used for evaluating vaccination, sleep, and parental care burden, which includes daily activity and social interaction, rehabilitation requirements, hearing, mood, and development. It has been proposed to detect post-intensive care syndrome (PICS) in children. This study aimed to outline the incidence of PICS in children using the VSCAREMD model and to describe the associated factors.
Methods
All children ages 1 month to 15 years and admitted to the intensive care unit for at least 48 hours were evaluated using the VSCAREMD model within 1 week of intensive care discharge. Abnormal findings were assorted into four domains: physical, cognitive, mental, and social. Descriptive statistics were performed using chi-square, univariate, and multivariate analyses.
Results
A total of 78 of 95 children (82.1%) had at least one abnormal domain. Physical, cognitive, mental, and social morbidity were found in 64.2%, 26.3%, 13.7%, and 38.9% of the children, respectively. Prolonged intensive care unit stay greater than 7 days was associated with dysfunction in physical (adjusted odds ratio [aOR], 3.80; 95% confidence interval [CI], 1.31–11.00), cognitive (aOR, 10.11; 95% CI, 3.01–33.89), and social domains (aOR, 5.01; 95% CI, 2.01–12.73). Underlying medical conditions were associated with cognitive (aOR, 13.63; 95% CI, 2.64–70.26) and social morbidity (aOR, 2.81; 95% CI, 1.06–7.47).
Conclusions
The incidence of PICS using the VSCAREMD model was substantially high and associated with prolonged intensive care. This model could help evaluate PICS in children.
INTRODUCTION
Millions of children around the globe suffer from critical illnesses that necessitate pediatric intensive care unit (PICU) admission. These critically ill children require lifesaving interventions to prevent mortality. With advancements in medicine, mortality has been significantly reduced over the years, although morbidity remains a concern. Substantial numbers of patients developed post-intensive care syndrome (PICS) after PICU discharge [1,2]. PICS was defined as new or worsening health problems arising after critical illness. These problems can involve physical, cognitive, mental, and emotional well-being and can affect the family caring for these critically ill children. The effects of such problems can persist beyond hospitalization [1-3]. Several previous prospective and descriptive studies were conducted to illustrate the burden of physical, cognitive, and mental problems in PICU survivors [4-12].
Despite numerous studies conducted to illustrate the impact of PICS in pediatric patients (PICS-p), there are several problems with the research. First, it is difficult to establish an accurate preadmission baseline in each child. Second, children have heterogeneous results compared to the adult population due to diverse functional statuses related to age and developmental stage. Moreover, with vast differences in measurement tools and follow-up timing among studies, no simple comprehensive model encompassing every domain of PICS-p can be used for evaluation of children across age groups.
The novel comprehensive VSCAREMD model was proposed by the pediatric intensivists and critical care nurses of the participating center. This model was utilized to conduct surveillance and detect the burden of PICS in children after PICU discharge beginning in February 2019. VSCAREMD is an acronym of seven validated tools to evaluate vaccination status (V), sleep problem (S), parental care burden (C), daily activity, social interaction (A), rehabilitation requirements (R), hearing problems (E), mood and behavior (M), and developmental problems (D) (Table 1) [13-22]. Abnormal findings are sorted into four domains: physical, cognitive, mental, and social. Each parameter of each domain within the model is generated in an attempt to cover all the aspects of post-intensive care problems mentioned in previous studies [3,4,23]. Vaccination surveillance was added to the model due to possible incomplete vaccination after prolonged hospitalization, which is highly probable in children admitted to the PICU. Nevertheless, data regarding the incidence of PICS after surveillance are lacking. Thus, this study aimed to outline the incidence of PICS in children using the VSCAREMD model and to describe the associated factors.
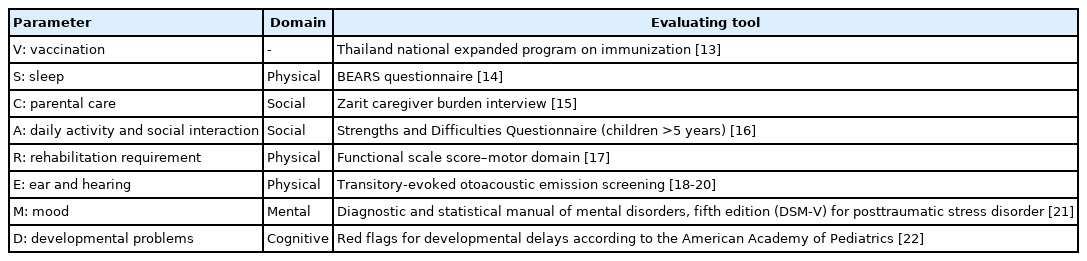
VSCAREMD model for evaluation of post-intensive care syndrome in children
MATERIALS AND METHODS
Study Design
This study was a retrospective chart review cohort study. The Ethics Committee of the Faculty of Medicine, Thammasat University approved the study. Due to the study’s retrospective nature, informed consent was waived.
Participants
All patients ages 1 month to 15 years who were admitted to the PICU for at least 48 hours from February 2019 to December 2019 were included in the analysis. The study was conducted in a large tertiary-care, university hospital with approximately 30–40 PICU admissions per month. The PICU at the center is a six-bed mixed surgical and medical intensive care unit. Patients with incomplete data on chart review were excluded.
VSCAREMD Model
As previously mentioned, there was no comprehensive model encompassed every domain of PICS-p. The VSCAREMD model was proposed based on discussion between pediatric intensivists and pediatric intensive care nurses at the center to identify the incidence of PICS in critically ill children after PICU discharge. The model was implemented in February 2019 as a part of the quality improvement service and was used as a service screening for every child discharged from the PICU. Pediatric residents were trained by the attending pediatric intensivist in terms of the assessment tools within the model before implementation. Four morbidity domains were graded based on featured parameters, as in Table 1. All evaluations were conducted by pediatric residents and attending pediatric intensivists within 1 week of PICU discharge. All abnormalities identified by the residents were confirmed by the attending intensivist.
Physical Domain
This domain included sleep problems (S), rehabilitation requirements (R), and hearing dysfunction (E). Sleep problems were assessed using the BEARS questionnaire [14]. Disturbances in sleep reported by either parents or children were considered. Rehabilitation requirements were evaluated using the functional scale score (FSS) in the motor domain [15]. Patients were then classified into one of five categories: normal function, mild dysfunction (one limb is functionally impaired), moderate dysfunction (two or more limbs are functionally impaired), severe dysfunction (poor head control), and very severe dysfunction (diffuse spasticity and paralysis). Any dysfunction noted by the FSS was considered. A transitory evoked otoacoustic emission (TEOAE) was used in the screening of abnormal hearing responses [18-20] and was measured by certified audiologists using Sentiero TEOAE (Screening/Diagnostic) (Path Medical, Germering, Germany). The nonlinear protocol was used at the stimulus level of 85 dB peak equivalent sound pressure. Absence of cochlear response was reported as “Refer” and was recorded as abnormal. Patients with abnormal results in any of the parameters were recorded as having abnormal physical domain.
Cognitive Domain
The cognitive domain was assessed using red flags for developmental delays (D) according to the American Academy of Pediatrics (AAP) [22]. Children who showed any red flag for developmental delay were considered to have cognitive problems. School-aged children and adolescents who had appropriate behavior and development for their age were considered to have normal cognition.
Mental Domain
The mental domain was mainly focused on the symptoms of post-traumatic stress disorder (PTSD) (M). All children surviving PICU were assessed for PTSD in the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-V) [21]. Any child who exhibited symptoms of PTSD such as intrusion, avoidance, or negative alterations in cognition and moods was considered abnormal, even if they had not yet fulfilled the 1-month criteria for diagnosis of PTSD.
Social Domain
The Zarit Caregiver Burden Interview was used to assess parental care burden in children surviving intensive care (C). A score exceeding 20 was considered significant [15]. In children older than 5 years, the Strengths and Difficulties Questionnaire (SDQ) was used to evaluate daily activity and social interaction (A) [16]. In younger children, activity was assessed by interviewing the parents as to whether the child could perform appropriately for their age in the activities of daily living and social interaction.
Vaccination
Vaccination problems (V) were also an important issue in pediatric patients and were assessed in this study. Missing vaccinations according to the Thailand National Expanded Program on Immunization based on age was considered incomplete [13].
Data Collection
As a quality improvement service, the results of the VSCAREMD model were recorded in each patient’s medical record. All demographic data, underlying conditions, admission diagnosis, ventilator support days, sedation and neuromuscular blocking agent used, PICU length of stay, and hospital length of stay were collected for analysis.
Statistical Analyses
Demographic data, incidence of abnormalities detected within each parameter and domain, and other quantitative data were described using median and percentage. Categorical data were analyzed using chi-square tests. Univariate and multivariate logistic regressions were used to determine the associated factors for each PICS domain. Crude and adjusted odds ratios (aORs) were reported along with the 95% confidence interval (CI). A P-value <0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS version 24.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Demographic Data
A total of 278 children was admitted to the PICU during the study period. Of these, 180 were excluded for PICU stay less than 48 hours, and another three children were excluded due to incomplete data. Thus, 95 children were included in the final analysis. The demographic data are summarized in Table 2. A total of 55 children (57.9%) in the cohort was male. The median age of the cohort was 2.0 years old (interquartile range [IQR], 0.2–5.0). The majority of children (61.1%) had underlying comorbidities, most with underlying cardiac conditions (30.5%). The most common admission diagnoses were cardiac disease (mainly postoperative cardiac surgery and congestive heart failure, 41%) and respiratory disease (mainly pneumonia and respiratory failure, 28.4%). The median Pediatric Risk for Mortality (PRISM) III was 2.0 (IQR, 0.0–6.0) [24]. Sixty-two children (62.3%) were mechanically ventilated with median ventilator days of 4.5 (IQR, 2.0–10.0). Twenty-two children (23.2%) were mechanically ventilated for more than 7 days. Sedation and neuromuscular blocking agents were used in 40 children (40.2%) and 18 children (18.9%), respectively. The median PICU stay was 5.0 days (IQR, 3.0–11.0). Prolonged PICU stays greater than 7 days were documented in 37 children (38.9%). The median day of evaluation after PICU discharge was 3.0 days (IQR, 2.0–4.0). A total of 78 children (82.1%) had at least one abnormal domain. The problems in each parameter and domain are described in Table 2.

Demographic data
Physical Domain
A total of 61 children (64.2%) had at least one abnormality within the physical domain parameters. Thirty-nine children (41.1%) reported having sleep problems using the BEARS questionnaire. FSS detected motor dysfunction in 33 children (34.7%) and abnormal TEOAE responses were reported in 19 children (20.0%). Among 33 children with motor dysfunction, seven showed mild dysfunction (21.2%), 11 moderate (33.3%), five severe (15.2%), and 10 very severe dysfunction (30.3%). Using univariate analysis, underlying comorbidities, prolonged PICU stays greater than 7 days, and mechanical ventilator support were associated with abnormalities in the physical domain, with the crude OR of 2.49 (95% CI, 1.05–5.90; P=0.037), 4.82 (95% CI, 1.75–13.30; P=0.001), and 3.45 (95% CI, 1.42–8.41; P=0.005), respectively. Sex, use of sedation, and neuromuscular blocking agents were not associated with physical domain dysfunction. After adjustment for statistically significant factors, prolonged PICU stay greater than 7 days was significantly associated with physical domain dysfunction with an aOR of 3.80 (95% CI, 1.31–11.00; P=0.014). Univariate and multivariate logistic regression analyses for the physical domain are summarized in Table 3.

Associating factors for physical domain dysfunction after PICU discharge
Cognitive Domain
Cognitive dysfunction was reported in 25 children (26.3%). Children with underlying disease revealed a significantly higher proportion of cognitive dysfunction (92.0% vs. 50.0%, P<0.001) with a crude odds ratio of 11.5 (95% CI, 2.52–52.53). Prolonged PICU stays of greater than 7 days and mechanical ventilation again demonstrated a significant association with cognitive problems with a crude OR of 9.15 (95% CI, 3.16–26.48; P<0.001) and 3.71 (95% CI, 1.15–11.97; P=0.022), respectively. Sex and the utilization of sedatives and neuromuscular blocking agents were not significantly related to cognitive dysfunction. From multivariate analysis, children with underlying conditions and children who were admitted to the PICU for longer than 7 days were significantly associated with cognitive problems (Table 4). Among 25 children with cognitive impairment, 12 (48.0%) were diagnosed with genetic comorbidities. Thus, a post hoc analysis was conducted after exclusion of patients with underlying genetic conditions that might have developmental delays; underlying diseases and prolonged PICU stay were still significantly correlated with cognitive dysfunction after PICU discharge, with a crude OR of 5.50 (95% CI, 1.13–26.64; P=0.020) and 9.63 (95% CI, 2.38–38.94; P≤0.001), respectively. A multivariate post hoc analysis revealed similar results that underlying comorbidities and prolonged PICU stay were associated with cognitive dysfunction, with an aOR of 6.84 (95% CI, 1.27–36.94; P=0.025) and 11.26 (95% CI, 2.59–48.87; P≤0.001), respectively.

Associating factors for cognitive domain dysfunction after PICU discharge
Mental and Social Domains
A total of 13 children (13.7%) exhibited PTSD symptoms during the study period based on the DSM-V criteria. Unlike the other domains, mechanical ventilation was shown to have a negative association with mental domain dysfunction with an OR of 0.27 (95% CI, 0.08–0.92; P=0.029) (Table 5). No multivariate analysis was performed in this domain due to only one statistically significant factor.
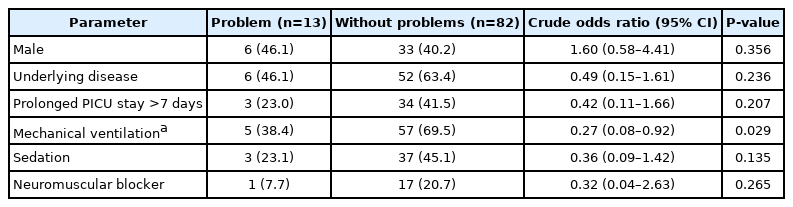
Associating factors for mental domain dysfunction after PICU discharge
In the social domain, 37 children (38.9%) were reported to have at least one parameter of dysfunction (Table 6). In terms of screening for parental burden, the Zarit Caregiver Burden Interview detected six children (6.3%) whose parents reported a significant burden. Thirty-four children (35.8%) had abnormal screening results for daily activity and social interaction using the SDQ questionnaire. Underlying comorbidities and prolonged PICU stay greater than 7 days were significantly associated with the development of social dysfunction after PICU discharge. Using multivariate analysis, both factors still demonstrated a statistically significant correlation with social domain dysfunction (Table 6).

Associating factors for social domain dysfunction after PICU discharge
Vaccination
Incomplete vaccination was found in 26 children (27.4%). Prolonged PICU stay was associated with incomplete vaccination with a crude OR of 2.91 (95% CI, 1.51–7.37; P=0.021) (Table 7). Since there was only one statistically significant risk factor, no multivariate analysis was performed.

Associating factors for incomplete vaccination after PICU discharge
DISCUSSION
To the authors’ knowledge, this study was the first epidemiological study of PICS in children in Thailand. The study found a substantially high prevalence of PICS-p development after PICU discharge. A total of 78 of 95 children (82.1%) had dysfunction in at least one domain. Sixty-one children (64.2%) had physical morbidity. After intensive care discharge, cognitive morbidity, mental morbidity, and social morbidity were found in 26.3%, 13.7%, and 38.9%, respectively.
The incidence of physical domain dysfunction after PICU discharge was similar to that found in previous studies, with a rate of 64% in this study compared to 8%–73% in the other studies [5-8]. A total of 34.7% of the children in this cohort demonstrated signs of motor impairment, comparable to the previous studies mentioned. Like the study by Inoue et al. [4], prolonged mechanical ventilation was associated with the development of physical dysfunction. This was due to excitation-contraction uncoupling and muscle biogenetic failure during critical illness [23]. Immobilization during mechanical ventilation could also play a role in the development of physical dysfunction [4].
This study revealed an incidence of 26.3% for cognitive dysfunction. Previous studies by Als et al. [8,9] revealed that children surviving critical illness scored lower on neuropsychologic and school performance measures that persisted until 12 months post-intensive care discharge. Another study by Ong et al. [2] demonstrated new cognitive problems in 3%–73% of PICU survivors using the Pediatric Cerebral Performance Category. The reason for the differences in incidence among the studies may be the various evaluation tools utilized. The Children Memory Scale implemented in the studies by Als et al. [8,9] was limited to children and adolescents ages five to 16 years and is not suitable for young children. Furthermore, the test consists of four batteries of subtests, which were time-consuming and required a high level of expertise [25]. This might not be suitable as a screening tool in young children, especially in the acute setting within 1 week of PICU discharge. In this cohort, the median age of the participants was relatively young at 2 years, and most of the children in the PICU were younger than 5 years; thus, red flags for developmental delays using the AAP guidelines were chosen as a screening tool. This can be conducted by the pediatric residents with the confirmation of attending general pediatricians or pediatric intensivists. Since the main objective was to screen patients with abnormal cognition within 1-week post ICU discharge, school-aged children and adolescents with appropriate for age developmental milestones were considered to have normal cognition in this study.
This study revealed that underlying comorbidities and prolonged PICU stay were significantly associated with the development of cognitive problems. After excluding children with genetic disease in the post hoc analysis, underlying diseases and prolonged PICU stay were still significantly correlated with cognitive dysfunction after PICU discharge. This study’s results coincided with a study by Peterson-Carmichael and Cheifetz [26] that found children with prolonged intensive care stays were at increased risk for developmental impairment compared to the general pediatric population.
In the mental domain, the incidence of children exhibiting PTSD symptoms in this study was comparable to other previous studies (13.7% vs. 13.8–34.5%) [10-12]. Interestingly, the use of mechanical ventilation seemed to be a protective factor against PTSD symptoms, with an OR of 0.27 (95% CI, 0.08–0.92; P=0.029). The authors hypothesize that it might be due to the sedation and pain control administered during mechanical ventilation. This is unlike a previous study by Herrup et al. [3], which demonstrated that septic illness, increased numbers of invasive procedures and interventions, and high dose narcotics and benzodiazepines were risk factors for mental dysfunction. However, with appropriate dosing of pain control during mechanical ventilation, patients might experience less pain during invasive procedures. Furthermore, sedatives could also have an amnestic effect, leading to less recall of the painful experience in the PICU. Despite the established risk of high-dose opioids and benzodiazepines on the mental problems of children surviving intensive care, adequate pain control and sedation were still imperative in caring for critically ill children. Since this study assessed patients within 1 week after ICU discharge, this might not fulfill the criteria for diagnosis of PTSD, which requires persistence of symptoms for more than 1 month [21]. Long-term follow-up of these patients is warranted to determine the true incidence of PTSD.
The incidence of reported social dysfunction in this cohort was relatively high at 38.9%. Approximately one-third of the children reported having abnormalities in daily activity and social interaction within 1 week of PICU discharge. A review by Inoue et al. [4] revealed that 36% of critically ill children’s family members experienced burden or overload. This was higher than the 6% revealed in the present cohort. The explanation for this difference might be the timing of evaluation. In this study, the parents were evaluated at 1 week after PICU discharge compared to 2 months in the review by Inoue et al. [4]. At 1 week after PICU discharge, parents might not be able to grasp the full impact of the burden of the critical illness. Long-term follow-up of critically ill parents might be warranted for evaluation of parental burden.
This study revealed that the VSCAREMD model could serve as a comprehensive tool to help detect the PICS-p after PICU discharge. Despite this usefulness, several limitations must be noted. This study was conducted as a single-center study in a tertiary care, university hospital, and the results might not represent the extensive impact of PICS-p in critically ill pediatric patients in generalized settings. Furthermore, the study aimed to explore the incidence of PIC-p within 1 week of PICU discharge and might not reflect the long-term impact of critical illness in these children. A longitudinal study is necessary to elucidate the long-term impact of critical illness in all aspects of PICS-p. Due to the relatively young age of the children included in this study, the results might not fully reflect the incidence of PICS in the PICU, which includes older patients. This study also did not explore other risk factors such as delirium and withdrawal, which might also impact cognitive and mental health [21]. Furthermore, delirium could also affect the test results of cognitive dysfunction such as SDQ and AAP red flags, which might also serve as another limitation of this study.
In conclusion, the incidence of PICS-p in each domain using the VSCAREMD model was substantially high and mostly highly associated with prolonged PICU stay of greater than 7 days. The VSCAREMD model could be utilized for detecting post-intensive care problems during follow-up after being discharged from the PICU.
KEY MESSAGES
▪ Physical, cognitive, mental, and social morbidity were found in 64.2%, 26.3%, 13.7%, and 38.9% of the children, respectively.
▪ Prolonged intensive care stay greater than 7 days was associated with post-intensive care syndrome.
▪ The incidence of post-intensive care syndrome in children using the VSCAREMD model was high and associated with prolonged intensive care stays.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING
None.
ACKNOWLEDGMENTS
The authors would like to show great appreciation to all the staff and faculty members of the participating hospital for the strong support and extensive cooperation. They also would like to express their gratitude to all parents and children participating in this study.
AUTHOR CONTRIBUTIONS
Conceptualization: CC. Data curation: all authors. Formal analysis: all authors. Methodology: CC. Project administration: all authors. Writing–original draft: all authors. Writing–review & editing: all authors.