Prevention and management of delirium in critically ill adult patients in the intensive care unit: a review based on the 2018 PADIS guidelines
Article information

Abstract
Delirium is an acute, confusional state characterized by altered consciousness and a reduced ability to focus, sustain, or shift attention. It is associated with a number of complex underlying medical conditions and can be difficult to recognize. Many critically ill patients (e.g., up to 80% of patients in the intensive care unit [ICU]) experience delirium due to underlying medical or surgical health problems, recent surgical or other invasive procedures, medications, or various noxious stimuli (e.g., underlying psychological stressors, mechanical ventilation, noise, light, patient care interactions, and drug-induced sleep disruption or deprivation). Delirium is associated with a longer duration of mechanical ventilation and ICU admittance as well as an increased risk of death, disability, and long-term cognitive dysfunction. Therefore, the early recognition of delirium is important and ICU medical staff should devote careful attention to both watching for the occurrence of delirium and its prevention and management. This review presents a brief overview of delirium and an update of the literature with reference to the 2018 Society of Critical Care Medicine Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU.
DEFINITION
The American Psychiatric Association (in the Diagnostic and Statistical Manual of Mental Disorders, fifth edition) defines delirium based on the following five criteria: (1) disturbance in attention (i.e., a reduced ability to direct, focus, sustain, and shift attention) and awareness; (2) a disturbance that develops over a short period of time (usually hours to days), represents a change from baseline, and tends to fluctuate during the day; (3) an additional disturbance in cognition (e.g., memory deficit, disorientation, language, visuospatial ability, or perception); (4) a disturbance that is not better explained by another preexisting, evolving, or established neurocognitive disorder and which does not occur in the context of a severely reduced level of arousal, such as coma; and (5) when there is evidence from medical or familial history, physical examination, or laboratory tests that the disturbance is caused by a medical condition, substance intoxication or withdrawal, or medication side effect [1]. Symptoms are often accompanied by sleep disturbance, abnormal psychomotor activity, and emotional disturbance.
Delirium is further differentiated according to the level of alertness; the motoric subtypes consist of the hyperactive, hypoactive, and mixed subtypes [2]. Patients with hyperactive delirium are aggressive, agitated, hallucinative, deluded, and exhibit increased psychomotor activity. In comparison, patients with hypoactive delirium have reduced alertness, lethargy, decreased responsiveness, and slowed motor skills. Patients with mixed subtypes of delirium fluctuate between hyperactive and hypoactive delirium. In the intensive care unit (ICU) setting, the prevalence values for the different subtypes of delirium are 1.6% for the hyperactive subtype, 43.5% for the hypoactive subtype, and 54.1% for the mixed subtype [2-4]. However, hypoactive delirium can easily be missed; more than 76% of total cases of hypoactive delirium are overlooked in the absence of a routine delirium screening. Study results indicate that the prognosis of delirium varies by subtype [5-7].
CLINICAL SIGNIFICANCE OF ICU DELIRIUM
ICU delirium is a predictor of increased mortality, prolonged hospital stay and mechanical ventilation, and greater costs as well as increased risks of reintubation and of transferring the affected patient to a long-term health care facility [8-11]. Delirium has an adverse impact on the post-discharge life of patients. Patients who had prolonged delirium showed poorer global cognition after discharge and greater risks of dementia and long-term cognitive impairment regardless of the severity and duration of their delirium [12-14].
RISK FACTORS
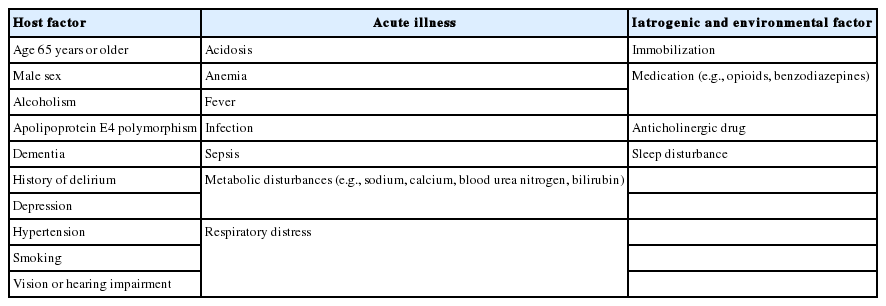
The causes of delirium are multifactorial. Risk factors can be separated into predisposing factors and precipitating factors (Table 1) [15]. Age is one of the most important risk factors associated with delirium in the ICU [16,17]. Other major host factors include previous dementia, hypertension, chronic illness, poor nutrition, substance withdrawal, tobacco use, and depression. Iatrogenic and other potentially modifiable factors include hypoxia, metabolic and electrolyte imbalances, infection, dehydration, hyperthermia, sepsis, psychoactive medications, a preceding period of sedation, coma, mechanical ventilation, and sleep deprivation [18-22]. Environmental variables that increase the risk of developing delirium in the ICU include isolation, absence of visits, absence of visible daylight, transfer from another ward, immobility, and the use of physical restraints [23,24]. Among the medications used for sedation during ICU care, benzodiazepines have been identified as an independent risk factor for the development of delirium [17,24,25]. However, evidence of an association between the use of opioid medications and the development of delirium remains inconsistent [9].
Postoperative delirium is a well-researched topic. Perioperative risk factors for delirium include intraoperative blood loss, transfusion, low hematocrit, pain, preoperative atrial fibrillation, and a longer surgery time [26-30]. Delirium is associated with high perioperative plasma cortisol levels in patients undergoing coronary artery bypass graft surgery and systemic corticosteroid treatment in patients with acute lung injury [31,32]. Among medications used in the ICU, antihistamines and furosemide can cause delirium as a consequence of their central anticholinergic effects [8].
PATHOGENESIS
The biological basis of delirium and confusion remains poorly understood, in part because it is difficult to evaluate severely ill patients using conventional electrophysiologic tests, brain imaging, and neurotransmitter assays. Furthermore, proposed animal models of delirium are not well-developed or validated at this time. Despite these limitations, some important results about the pathophysiology of delirium have been reported to date.
First, imbalances or derangements of multiple neurotransmitter systems have been implicated in the pathophysiology of delirium. Cerebrospinal fluid studies of patients with delirium reveal alterations in neuropeptides [33]. Acetylcholine is one of the major neurotransmitters involved in ascending reticular activating system function and plays a key role in the pathogenesis of delirium [34]. A reduction in cholinergic function leads to increased levels of glutamate, dopamine, and norepinephrine in the brain. Decreased serotonin and gamma-aminobutyric acid levels also possibly contribute to the pathogenesis of delirium [35,36]. Anticholinergic drugs cause delirium when given to healthy volunteers and are even more likely to lead to acute confusion in the elderly [37]. With respect to hyper- or hypoactive delirium, dopamine excesses may contribute to hyperactive delirium, which has been linked with simultaneous acetylcholine decreases. Thus, acetylcholine and dopamine may be inversely related in delirium pathogenesis; pharmacological and neuroanatomical evidence also support this model [38]. Separately, norepinephrine plays an important role in modulating attention, anxiety, and mood; like dopamine, excess noradrenergic activity has been associated with hyperactive delirium [39].
Inflammatory mediators (e.g., cytokines, chemokines) are readily expressed during critical illness, trauma, and sepsis and following surgical intervention. Sepsis, severe sepsis, and septic shock are characterized by significantly elevated C-reactive protein, S-100β protein, and cortisol levels in patients with delirium versus without [40,41]. Proinflammatory cytokines (e.g., tumor necrosis factor-α, interleukin-1 family cytokines) and chemokines are associated with endothelial damage in the central nervous system, thrombin formation, and microvascular dysfunction; importantly, these events can result in delirium. A study of ICU patients found that higher levels of procalcitonin at the time of ICU admission are associated with prolonged durations of brain dysfunction. Trends in higher levels of C-reactive protein also suggest a possible association with delirium [42]. However, it is difficult to exclude the confounding effects of underlying illness or dementia.
RECOGNITION AND DIAGNOSIS OF DELIRIUM
Delirium is common in critically ill adults [3,4]. However, the use of ICU delirium screening tools appears to be uncommon. For example, only 53% of ICU nurses perform delirium assessments [43]. Early recognition of delirium is important, if only to avoid prolonging its duration due to exacerbation by iatrogenic factors. Clinicians must employ tools that allow for a timely, accurate assessment of patients in various settings to be completed. Recognition is more difficult in the ICU setting because a patient may have a purposefully altered sensorium secondary to the sedation administered for procedures, pain control, or mechanical ventilation. Therefore, the assessment of a patient for delirium in the ICU is a two-step process because the clinician must first determine the current level of sedation before the actual assessment can be performed. Scales that can be used to assess sedation include the Ramsay Sedation Scale [44], the Riker Sedation-Agitation Scale [45], and the Richmond Agitation–Sedation Scale (RASS) [46,47].
It is appropriate for the clinician to check for the presence of delirium after the level of sedation has been determined and the patient is deemed responsive to a verbal stimulus. Multiple instruments have been validated for use in non-ICU patients, but only two are validated for the diagnosis of delirium in mechanically ventilated patients (i.e., the intensive care delirium screening checklist [ICDSC] [48] and the confusion assessment method for the ICU [CAM-ICU] [49]). A translated Korean version of CAM-ICU with proven high sensitivity and specificity is also available [50]. Use of the RASS for the assessment of sedation followed by the CAM-ICU or the ICDSC is one approach for the establishment of a delirium diagnosis in ICU patients. A diagnosis of delirium using the CAM-ICU requires (1) an acute change or fluctuation in mental status (feature 1); (2) inattention (feature 2); and (3) one of the following: (a) disorganized thinking (feature 3) or (b) an altered level of consciousness (feature 4). Importantly, though, only patients with a RASS score of three points or more are considered alert enough to respond to the CAM-ICU test and thus be assessed in this manner for delirium. Separately, when making a diagnosis using the ICDSC, patients who score at least four points are considered to have the condition.
Some studies have suggested that delirium evaluations should not be performed while the patient is sedated [51,52]. It is true that a small subset of patients (approximately 10%) may have rapidly reversible sedation-related delirium that dissipates after sedation is discontinued. Unfortunately, a study evaluating rapidly reversible delirium found that most patients continued to have persistent delirium even after sedation was interrupted. If possible, the assessment of delirium should be performed following sedation interruption. The evaluation of delirium should not be discontinued, because a low percentage of patients experience sedative delirium.
Laboratory evaluations of patients with delirium should include serum electrolyte, creatinine, glucose, and calcium concentrations as well as a complete blood count, urinalysis, and urine culture. Drug levels, toxicology screening, liver function testing, and arterial blood gas measurements should follow if the cause remains undetermined. Neuroimaging, lumbar puncture, and electroencephalography (EEG) are not required in most patients with delirium; however, they are recommended in specific clinical scenarios, including in efforts to elucidate delirium causes that remain obscure after routine testing. EEG is also useful in patients with altered consciousness to exclude seizures, especially nonconvulsive or subclinical seizures, and to confirm the diagnosis of specific metabolic encephalopathies or infectious encephalitides that have characteristic EEG patterns [53,54].
PREDICTION
The early recognition of delirium is important for critically ill patients in the ICU. Predictive models that include delirium risk factors at the time of ICU admission and during the 24 hours after ICU admission have already been validated. The Prediction of Delirium in ICU Patients (PRE-DELIRIC) model uses 10 predictors—specifically, age, Acute Physiology and Chronic Health Evaluation II score, admission group, urgent admission, infection, coma, sedation, morphine use, urea level, and metabolic acidosis—and has an area under the receiver operating characteristic (AUROC) curve value of 0.77 (95% confidence interval [CI], 0.74 to 0.79) [55]. In comparison, the early (E)-PRE-DELIRIC model uses nine predictors (age, history of cognitive impairment, history of alcohol abuse, blood urea nitrogen, admission category, urgent admission, mean arterial blood pressure, use of corticosteroids, and respiratory failure) and has an AUROC curve value of 0.76 (95% CI, 0.73 to 0.77) [56]. Because the PREDELIRIC and E-PRE-DELIRIC models have similar predictive values, the decision of which model to choose can be based on the availability of information about predictors. Both models are based on screening using only the CAM-ICU.
PREVENTION AND MANAGEMENT
The Society of Critical Care Medicine recently issued the 2018 Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU (PADIS) [57]. Compared with the 2013 guidelines [9], these new 2018 guidelines include two inextricably-related clinical care topics (immobility and sleep), involved patients as collaborators and coauthors, and invited panelists from high-income countries to include insights from diverse practices and expertise from the global critical care community. It is believed that these factors will promote opinions from the guidelines to be more effectively applied in clinical practice.
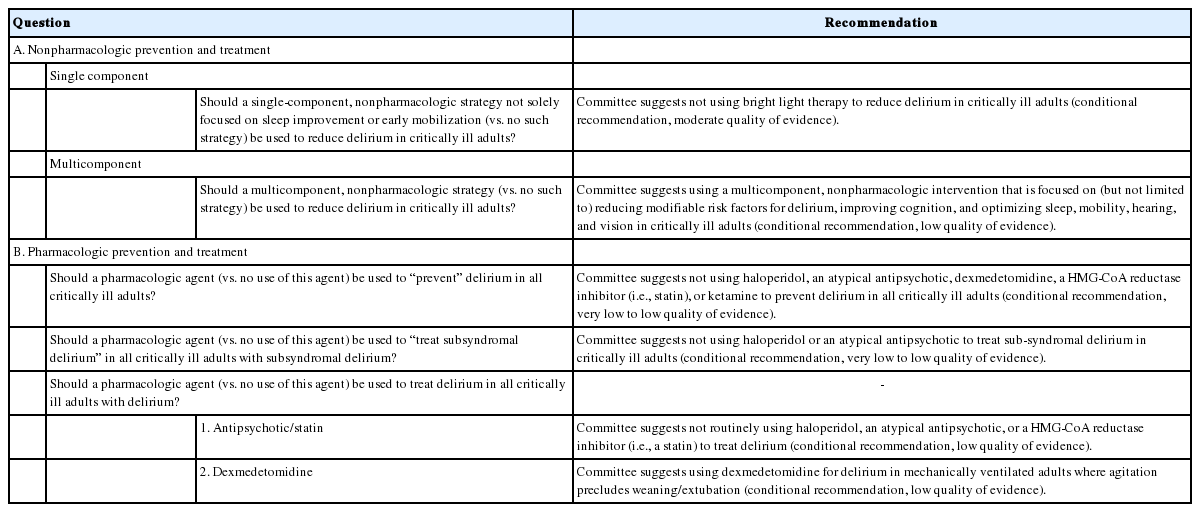
Critically ill adults should be regularly assessed for delirium using a valid tool and predictive models [55,56] that include delirium risk factors at the time of ICU admission and during the first 24 hours thereafter. These tools have been validated and can be used to predict delirium in critically ill adults. Table 2 presents a summary of the questions and recommendations (and the strength of evidence for each) for delirium prevention and management included in the 2018 PADIS guidelines [57].
Nonpharmacologic Prevention and Treatment
Most ICUs employ nonpharmacologic methods to reduce or prevent delirium. Regularly allaying anxiety and orienting patients, reducing environmental noise and the use of alarms, establishing light use consistent with day–night circadian cycles, and encouraging early mobility are some examples of strategies. A before-and-after study found that the use of a delirium monitoring/management and early exercise/mobility bundle (i.e., awakening and breathing coordination, delirium monitoring/management, and early exercise/mobility [ABCDE]) was significantly associated with reduced delirium in patients [58]. A revised and expanded ABCDEF bundle that included a different focus on “A” (assessment and treatment of pain) and the addition of “F” (family engagement) was evaluated using a large, multicenter, before-and-after cohort study. In this study, delirium was also assessed using the CAM-ICU. The adjusted analysis revealed that improvements in bundle compliance were significantly associated with reduced mortality rates and more ICU days without coma or delirium [59].
Disruption of the sleep–wake cycle in the ICU is another risk factor for delirium. When possible, maintaining an optimal sleep–wake cycle using either nonpharmacologic or pharmacologic means may help to prevent delirium [60].
Pharmacologic Prevention and Treatment
There is no evidence available to date that the routine use of antipsychotic therapy for the treatment of delirium is efficacious [61-64]. The Haloperidol Effectiveness in ICU Delirium trial found no benefit of treatment with haloperidol. However, such may be considered in the treatment of acute agitation (hyperactive delirium) [61]. Use of all antipsychotic agents should be discontinued immediately following the resolution of the patient’s distress symptoms. The committee suggests not using haloperidol, an atypical antipsychotic; dexmedetomidine, a β-hydroxy β-methylglutaryl-coenzyme A reductase inhibitor (i.e., statin); or ketamine to prevent delirium in critically ill adults, although this is a conditional recommendation with a very low to low quality of evidence. The committee also recommends avoiding routinely employing the above pharmacologic agents (conditional recommendation, low quality of evidence) and using dexmedetomidine for the treatment of delirium in mechanically ventilated adults who have agitation that precludes weaning/extubation (conditional recommendation, low quality of evidence). Recommendations for delirium treatment strategies suggest that the application of dexmedetomidine may be a better treatment strategy than one that is based on benzodiazepine administration. A single-cohort randomized trial evaluated dexmedetomidine’s role as a treatment for agitation precluding ventilator liberation [65].
Dexmedetomidine is a highly selective, centrally acting alpha-2-agonist with anxiolytic, sedative, and some analgesic effects. It has no deleterious effects on respiratory drive. An initial loading dose is typically not performed, but can be administered if necessary [66]. The initial loading dose may cause transient hypotension or hypertension, depending upon whether vasodilation from the activation of central alpha 2a receptors or vasoconstriction from the activation of peripheral alpha 2b receptors predominates. The usual dexmedetomidine maintenance dose is 0.2 to 0.7 μg/kg/hr, with dosage increases suggested to happen as needed not more frequently than every 30 minutes. There are no specific guidelines for modifying the dose for elderly patients or patients who have renal or hepatic impairment. It is prudent to start at the low end of the dosage range and titrate slowly in accordance with the patient’s response. The variability in patient response to dexmedetomidine may be due to as-yet-unidentified patient characteristics, pharmacokinetics, and genetic polymorphisms [67].
The results of another study indicated that prophylactic nighttime administration of dexmedetomidine results in a rate of ICU delirium prevention of 80% (compared with 20% using a placebo) during ICU admittance [68]. This randomized trial found that fewer of the patients who receive dexmedetomidine require a fentanyl infusion during their ICU stay (76% vs. 94%, respectively; P=0.02). Results obtained using the Leeds Sleep Evaluation Questionnaire indicated that sleep quality was no different between the dexmedetomidine and placebo groups. The lower proportion of patients requiring a fentanyl infusion during the ICU stay in the intervention group may be related to a dexmedetomidine-associated analgesic effect; the rates of fentanyl infusion at the time of randomization were frequent and similar between the two groups. These potential coanalgesic and opioid-sparing effects merit further study given the increasing concerns about opioid consumption during hospitalization.
CONCLUSIONS
Delirium is a disturbance of consciousness and cognition that occurs during a short period of time. It is associated with significantly increased morbidity and mortality rates in critically ill patients. Subtypes of delirium include hyperactive, hypoactive, and mixed. Many risk factors are associated with delirium; some are modifiable or preventable by the clinician. There are multiple validated assessment tools available to evaluate delirium. Patients in the ICU must first be assessed for sedation levels and then for the presence of delirium, using scales such as the CAM-ICU or the ICDSC.
Minimizing sedation using tactics such as daily interruptions of sedation can help to reduce exposure to delirogenic psychoactive medications. The application of benzodiazepines should be avoided in the ICU, except for the treatment of specific conditions. Alternatives available for sedation include haloperidol, atypical antipsychotics, dexmedetomidine, and remifentanil. However, additional pharmacologic intervention studies should be performed to determine the roles of these medications in the prevention and treatment of delirium.
KEY MESSAGES
▪ Delirium is common in critically ill adults. Minimizing sedation is important for the prevention of delirium.
▪ Use of benzodiazepines should be avoided in the intensive care unit, except for the treatment of specific conditions.
▪ Dexmedetomidine administration can be considered for delirium in mechanically ventilated adults where agitation precludes weaning/extubation.
Notes
CONFLICT OF INTEREST No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: HBL. Data curation: SYP. Formal analysis: SYP. Methodology: SYP, HBL. Project administration: HBL. Visualization: SYP. Writing - original draft: SYP, HBL. Writing - review & editing: HBL.