High-flow nasal cannula for respiratory failure in adult patients
Article information

Abstract
The high-flow nasal cannula (HFNC) has been recently used in several clinical settings for oxygenation in adults. In particular, the advantages of HFNC compared with low-flow oxygen systems or non-invasive ventilation include enhanced comfort, increased humidification of secretions to facilitate expectoration, washout of nasopharyngeal dead space to improve the efficiency of ventilation, provision of a small positive end-inspiratory pressure effect, and fixed and rapid delivery of an accurate fraction of inspired oxygen (FiO2) by minimizing the entrainment of room air. HFNC has been successfully used in critically ill patients with several conditions, such as hypoxemic respiratory failure, hypercapneic respiratory failure (exacerbation of chronic obstructive lung disease), post-extubation respiratory failure, pre-intubation oxygenation, and others. However, the indications are not absolute, and much of the proven benefit remains subjective and physiologic. This review discusses the practical application and clinical uses of HFNC in adults, including its unique respiratory physiologic effects, device settings, and clinical indications.
INTRODUCTION
Oxygen therapy is typically delivered via low-flow systems (e.g., nasal cannulae or masks) or high-flow systems (e.g., venturi masks or nonrebreathers). The high-flow nasal cannula (HFNC) is a unique mode of noninvasive respiratory support that delivers warmed, humidified oxygen with a fraction of inspired oxygen (FiO2) of 0.21 to 1.0 and a flow rate as high as 60 L/min. HFNC is indicated for patients with respiratory failure due to various underlying conditions.
The benefits of HFNC over conventional oxygen devices (low-flow systems [nasal cannulae or masks] and high-flow systems [Venturi masks]) and noninvasive ventilation (NIV; continuous or bilevel positive airway pressure ventilation) are improved patient comfort and physiologic advantages. The latter include improved oxygenation and ventilation, better pulmonary compliance, reduced anatomical dead space, modest positive end-expiratory pressure, more efficient respiratory effort, reduced work of breathing, and improved secretion clearance [1]. The goal of this review is to examine research on HFNC in adult patients, with an emphasis on its physiological effects, titration of the device, and varied clinical applications.
PHYSIOLOGIC EFFECTS
Supplemental oxygen therapy is the first-line therapy for respiratory failure. Generally, oxygen is provided via low-flow systems (nasal cannulae or masks). However, several disadvantages have been reported relative to high-flow systems, including low efficacy and low tolerance of oxygen delivery. Bubble humidifiers are commonly used with low-flow systems for spontaneously breathing patients, but because the absolute humidity is low, patients still report discomfort, especially dry nose, dry throat, and nasal pain [2,3]. Insufficient heating and humidification also result in poor compliance with these devices. Finally, with conventional treatments in patients with respiratory failure, a disparity exists between the delivered oxygen flow and the inspiratory flow of the patient. The oxygen flow is delivered at a maximum of 15 L/min, while the inspiratory flow in these patients ranges from 30 L/min to greater than 100 L/min. As a consequence of this large disparity, the fraction of inspired oxygen (FiO2) is variable and frequently lower than intended.
Gas from an air/oxygen blender is heated, actively humidified, and then delivered via a heated circuit. The blender can generate a flow as high as 60 L/min. The physiological effects of gas administered in this manner are outlined in Table 1.

Advantages and disadvantages of high-flow nasal cannula treatment
Anatomical Dead Space Washout
HFNC can flush out the expired carbon dioxide accumulated in the anatomical dead space of the nasopharynx. This decreased accumulation can improve the efficiency of ventilation and thoracoabdominal synchrony and enhance oxygen delivery [4-6]. Thus, improved washout with HFNC relative to other oxygen delivery systems permits a larger fraction of minute ventilation to participate in alveolar gas exchange.
Positive End Expiratory Pressure Effect
HFNC is an open system; however, the high rate of flow from the cannula resists expiratory airflow and elevates the airway pressure [7]. In adults, as in neonates and infants, HFNC has been shown to exhibit the “positive end expiratory pressure (PEEP) effect,” in which it raises the peak nasopharyngeal airway pressure present at the end of expiration [8-10], particularly when the mouth is closed. This “PEEP effect” can reduce the work of breathing, mitigate auto-PEEP (if present), and improve oxygenation. Each added increment of 10 L/min of oxygen flow adds approximately 0.7 cm H2O (up to approximately 3 cm H2O) of PEEP when the patient’s mouth is closed and 0.35 cm H2O when it is open [11].
Fraction of Inspired Oxygen
Physiologically, inspiratory flow and tidal volume vary breath-by-breath [12]. Patients with respiratory failure demand higher inspiratory flow rates that exceed the flow rates of standard oxygen supply devices, resulting in the entrainment of room air and a reduction in the FiO2 of the delivered gas. The FiO2 level varies during low-flow oxygen delivery and is generally much lower than predicted by equipment algorithms [13,14]. However, with HFNC, the gas flow rate to the patient is much higher than with low-flow oxygen systems. High flow rates minimize the entrainment of room air, yielding more accurate delivery of oxygen, especially relative to conventional delivery systems. Additionally, elevated flow rates have been demonstrated to lower the respiratory rate while increasing tidal volume, improving the overall pattern of breathing [9,15].
Humidification
HFNC ventilation systems typically include a heated humidifier. This allows these devices to deliver optimally heated and humidified gas to patients better than conventional oxygen systems. The added humidification increases the mucosal water content, aiding in the removal of secretions and potentially reducing the work of breathing. This also moistens the airway, avoiding the epithelial injury associated with airway desiccation [16,17].
Small Pliable Nasal Prongs (Comfortable Interface)
HFNC exhibits outstanding acceptance and tolerability resulting from its uniquely soft and pliable nasal prongs (Figure 1). As such, several studies have described greater patient comfort with HFNC than with conventional low-flow or high-flow oxygen administered through a face mask or nasal cannula [18-20]. NIV, in turn, is difficult to manage for extended durations, making HFNC an exciting potential alternative for do-not-intubate patients.
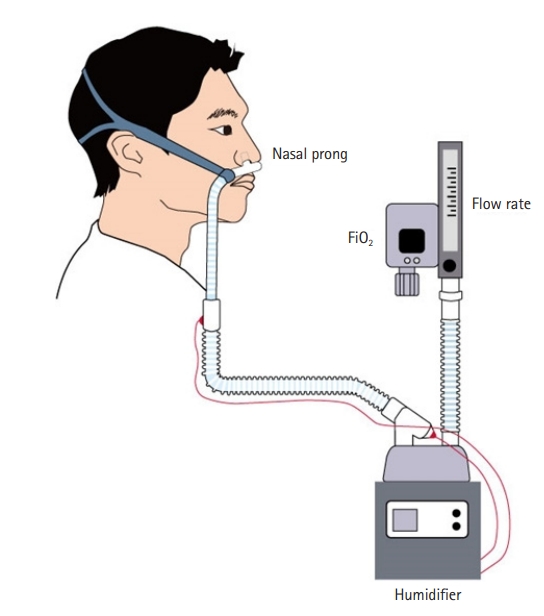
High-flow nasal cannula oxygen device. An air/oxygen blender, allowing a fraction of inspired oxygen (FiO2) from 0.21 to 1.0, generates flow up to 60 L/min. The gas is heated and humidified by an active heated humidifier used during mechanical ventilation. The patient breaths medical gas through a unique large-diameter pliable nasal cannula with a single-limb heated inspiratory circuit.
CLINICAL SETTINGS (DEVICE TITRATION)
HFNC is increasingly used to deliver oxygen to critically ill patients, especially those experiencing respiratory failure. However, no recommendations have been established for its practical application. Although HFNC can be administered on an unmonitored floor, it is usually applied in a monitored setting such as the intensive care unit (ICU), intermediate care wards, or emergency department [6,17].
Oxygen gas is adequately heated and humidified and is then delivered through a unique wide-bore nasal cannula, generally made of softer, more pliable plastic than the cannulae for low-flow systems. The cannula fits snugly into the snares and is held in place with a head strap (Figure 1).
Two parameters must be set: the flow rate and the FiO2. The flow rate should be set first, typically at 20 L/min to 35 L/min (range, 5–60 L/min). Second, the FiO2 (range, 21%–100%) is set to target a desired peripheral oxygen saturation. The flow rate can subsequently be increased in 5 to 10 L/min increments if the respiratory rate fails to improve, oxygenation fails to adequately improve, or breathing remains labored. Both increasing the flow rate and increasing the FiO2 will result in improved peripheral oxygen saturation. We recommend maximizing the flow rate first and attempting to keep the FiO2 ≤60%; however, an increase in FiO2 may be necessary to achieve adequate oxygenation.
HFNC is generally well tolerated and can be administered for several days. Patients can be switched to a low-flow system (nasal cannula or mask) once the flow rate reaches 20 L/minute or lower and FiO2 reaches 50% or lower.
CLINICAL APPLICATIONS
Acute Hypoxemic Respiratory Failure
HFNC versus low-flow oxygen
The indication of HFNC is supported by randomized trials and observational studies of patients with hypoxemic respiratory failure. While data are conflicting, these studies consistently demonstrate improved oxygenation and a decreased need for intubation when HFNC is used relative to low-flow oxygen systems [4,5,18,21-34]. However, studies have failed to show consistent and convincing benefits for mortality, length of ICU and hospital stay, dyspnea, and comfort.
The High Flow Nasal Oxygen Therapy in Resuscitation of Patients with Acute Lung Injury (FLORALI) trial was a large multicenter randomized study in which HFNC was compared with conventional oxygen therapy and NIV [22]. Adults with no prior history of lung disease and respiratory failure were randomly assigned to receive HFNC therapy, oxygen via a nonrebreather face mask, or NIV. Ultimately, the intubation rate (the primary endpoint) was similar among treatment modalities. However, other outcomes included 90-day mortality and ventilator-free days, both of which were notably lower among the patients treated with HFNC than in those treated with NIV or conventional oxygen therapy. In a post hoc examination, HFNC was also associated with lower intubation rates among patients with a partial pressure of oxygen (PaO2)/FiO2 ratio lower than 200. However, because overall intubation rates were lower than anticipated, the power of the study was insufficient to address this question. Finally, in examining whether delays in intubation that could influence treatment outcomes had been present, the authors concluded that the time to intubation did not differ significantly between HFNC and NIV.
Another important randomized trial involving HFNC was the Randomized Controlled Trial of Humidified High-Flow Nasal Oxygen for Acute Respiratory Distress in the Emergency Department; HOT-ER study, which described the early initiation of HFNC in 322 emergency room patients with hypoxemia. Compared with conventional oxygen therapy, the investigators found that HFNC was not superior [21]. HFNC was associated with lower intubation rates after 24 hours (HFNC, 5.5%; conventional oxygen treatment, 11.6%), although this disparity was not statistically significant (P=0.053). The groups exhibited similar 90-day mortality rates (HFNC, 21.2%; conventional oxygen treatment, 17.4%).
The conflicting results between the FLORALI and HOT-ER trials may relate to key differences in study design and patient characteristics, such as underlying comorbidities. In the FLORALI trial, the most common cause of respiratory failure was pneumonia (approximately 80% of patients). In contrast, in the HOT-ER study, only approximately one-fourth of patients had pneumonia. Additionally, over half of the HOT-ER study participants were diagnosed with asthma, heart failure, or chronic obstructive lung disease (COPD), diagnoses that were exclusion criteria for the FLORALI trial. In the FLORALI study, participants received 48 hours of continuous HFNC, while HOT-ER lacked any specific HFNC treatment protocol, potentially resulting in insufficient HFNC treatment in the latter study. HOT-ER also did not compare HFNC with NIV. In addition, the studies differed in the details of the high flow settings used; for instance, the flow rate was set 10 L/min lower in the HOT-ER than in the FLORALI protocol. Although a small disparity, the greater flow rate in the FLORALI study may have improved CO2 clearance among the participants, reducing the work of breathing and leading to fewer intubations.
In a meta-analysis of 14 trials, the authors compared HFNC with conventional oxygen therapy in patients with acute hypoxemic respiratory failure. HFNC treatment had little or no impact on the intubation rate (26% in both groups; odds ratio, 0.98; 95% confidence interval [CI], 0.34–2.82) or the mortality rate (26% for HFNC vs. 27% for conventional oxygen therapy; relative risk [RR], 0.97; 95% CI, 0.82–1.14) [35]. The same meta-analysis also reported reduced dyspnea and improved comfort among the HFNC group as well as a possible reduction in hospital-acquired pneumonia, but the effects on ICU admissions and length of stay were uncertain.
In another meta-analysis of nine trials that compared HFNC to low-flow oxygen in patients with hypoxemic respiratory failure, HFNC was associated with a decreased need for both intubation (RR, 0.85; 95% CI, 0.74–0.99) and escalation of respiratory support (RR, 0.71; 95% CI, 0.51–0.98) [36]. However, no differences were observed in the mortality rate, length of stay, or patient dyspnea and comfort.
Moreover, in a network meta-analysis, HFNC was shown to reduce the intubation rate in patients with acute hypoxemic respiratory failure compared with conventional low-flow oxygen, but no impact was observed on mortality (RR, 0.76; 95% CI, 0.55–0.99) [37].
HFNC versus NIV
Conflicting evidence exists about whether NIV is beneficial to patients with hypoxemic nonhypercapnic respiratory failure [38-46]. A network meta-analysis of 25 randomized trials examined outcomes in patients with acute hypoxemic respiratory failure who were treated with noninvasive modalities (helmet NIV, facemask NIV, and HFNC) compared with those of patients who were treated with low-flow oxygen [37]. Mortality was lower among patients treated with helmet or face mask NIV than in those treated with low-flow oxygen (helmet NIV: RR, 0.40; 95% CI, 0.24–0.6; face mask NIV: RR, 0.83; 95% CI, 0.68–0.99). All three noninvasive modalities were associated with lower intubation rates (helmet NIV: RR, 0.26; 95% CI, 0.14–0.46; face mask NIV: RR, 0.76; 95% CI, 0.62–0.90; HFNC; RR, 0.76; 95% CI, 0.55–0.99). However, this network meta-analysis should be interpreted with caution due to significant heterogeneity and risk of bias due to lack of blinding, as well as a wide range of etiologies for respiratory failure and illness severity among participants. In addition, the mortality benefit was not found among patients with severe hypoxemia (a PaO2/FiO2 ratio <200 mm Hg).
In a meta-analysis that included 29 randomized trials with mixed populations of participants who had acute respiratory failure, HFNC was compared with NIV [42]. HFNC was associated with lower rates of mortality (RR, 0.44; 95% CI, 0.24–0.79), intubation (RR, 0.71; 95% CI, 0.53–0.95), and possibly hospital-acquired pneumonia (RR, 0.46; 95% CI, 0.15–1.45) and improved patient comfort. However, interpretation of the analysis is limited by the small sample size and heterogeneity in the study design, patient population characteristics, type of respiratory failure, and outcomes. Despite these limitations, HFNC appears to be at least non-inferior and is an acceptable choice in this clinical setting.
With regard to devices, helmet NIV was compared with HFNC in another small study of severely hypoxemic patients [34]. Helmet NIV was associated with greater improvements in oxygenation, a reduction in dyspnea and respiratory effort, and similar levels of PaCO2.
Concerns have been raised regarding whether the use of HFNC can potentially delay necessary intubation and worsen outcomes [47]. As a result, when HFNC is used, clinicians should remain vigilant to signs of respiratory failure that necessitate intubation and mechanical ventilation. Patients who are not tachypneic may experience success with HFNC despite a relatively high FiO2. The ROX index (peripheral arterial oxygen saturation/fraction of inspired oxygen [expressed as a percentage]/respiratory rate) may also help guide clinicians in this regard. In one small series, a ROX index of >4.88 at 2, 6, and 12 hours after initiation of HFNC was shown to indicate a lower likelihood of subsequent endotracheal intubation. Further studies are needed to validate the value of ROX in this population before it can be routinely used.
Acute Hypercapnic Respiratory Failure
Hypercapnic respiratory failure is another frequent clinical situation that can arise from acute exacerbation of COPD. For patients with this condition, when other oxygen devices have failed, NIV has been the primary treatment for respiratory support before endotracheal intubation. However, because of poor mask compliance, it is inappropriate for some patients [48,49]. Among these patients with hypercapnic respiratory failure, since HFNC tends to be well-tolerated, it can frequently be utilized to manage the condition successfully [50].
Although HFNC does not provide active inspiratory support in COPD patients, the technique has been shown to increase tidal volume [51]. Nilius et al. [52] found varied effects of HFNC on hypercapnic respiratory failure from COPD; for some individuals, the frequency of breathing was depressed, while for others, PaCO2 was lowered. Among stable patients with COPD, HFNC also increases the capacity for exercise, providing improved oxygenation relative to spontaneous breathing [53]. These results suggest that, for certain forms of hypercapnic respiratory failure, HFNC is an extremely promising therapeutic option.
Pre-intubation Oxygenation
During intubation support, preoxygenation is routinely used to prevent desaturation. Most experts use conventional systems and bag-mask ventilation to deliver oxygen prior to intubation; the bag mask or oxygen mask is temporarily removed for the intubation procedure. Although not routine, HFNC is an acceptable method to provide oxygen to patients undergoing intubation, both before (preoxygenation) and during the procedure (to prevent desaturation). However, data regarding the value of HFNC for preoxygenation prior to intubation are conflicting [54-57].
Several trials have shown improved oxygenation when HFNC strategies are used. One randomized single-center study compared 4 minutes of preoxygenation with HFNC (100% FiO2 at 60 L/minute) together with concomitant NIV (10 cm H2O pressure support ventilation and 5 cm H2O PEEP) with NIV alone prior to intubation. HFNC/NIV was associated with higher peripheral oxygen saturation (100% vs. 96%) and fewer patients with episodes of desaturation below 80% (0% vs. 21%) [54]. Miguel-Montanes et al. [55] reported similar results in a study of 101 patients, where compared with a nonrebreather mask, peripheral oxygen saturation levels at the end of the preoxygenation period were higher with HFNC (100% vs. 94%) and fewer patients exhibited episodes of severe hypoxemia (2% vs. 14%). Overall, HFNC was associated with a significant decrease in the prevalence of severe hypoxemia, and the authors concluded that its application could improve the safety of patients while they are intubated in the ICU.
In contrast, in a multicenter study of 124 patients undergoing intubation who had severe hypoxemia (PaO2/FiO2 ratio <300 mm Hg, respiratory rate >30 breaths/min, and a FiO2 >50% to achieve a saturation of >90%), HFNC did not reduce the lowest saturation during intubation when compared with preoxygenation using a conventional high-flow oxygen face mask [56]. The discordant results may be explained by differences between the studies in the indications for intubation and severity of hypoxemia prior to intubation.
Post-extubation (Preventing Re-intubation)
Every patient should be oxygenated following extubation. For most patients, this goal is achieved with low-flow systems (nasal prongs or simple masks). When a higher-flow system is required, Venturi masks or HFNC may be applied. The choice of oxygen devices should be individualized and depends on factors including oxygen requirement, the etiology of respiratory failure, and patient preferences.
The efficacy of HFNC in the post-extubation periods was best illustrated in a trial of 527 patients (mixed postsurgical and medical) at low risk for reintubation following extubation. For 24 hours post-extubation, HFNC was associated with less frequent reintubations than occurred when conventional oxygen was used (4.9% vs. 12.2%), as well as improved secretion clearance, with 14 patients needed to treat to prevent 1 reintubation [57]. In patients at high risk for reintubation, HFNC and NIV were compared in a randomized trial of 604 patients (mixed surgical and medical populations). After 72 hours, 22.8% of the HFNC group required reintubation compared to 19.1% in the NIV group [58]. While the length of the ICU stay was lower in those treated with HFNC, no differences were observed in the rates of mortality, sepsis, or multiorgan failure. Additionally, although 20% of participants in this trial were patients with moderate to severe COPD, these data are insufficient to make a robust recommendation in favor of HFNC for patients with COPD with chronic hypercapnia, a population in which the evidence and guidelines favor NIV.
A meta-analysis of 9 trials reported that HFNC was associated with reduced reintubation rates (RR, 0.46; 95% CI, 0.30–0.70) and incidence of post-extubation respiratory failure (RR, 0.52; 95% CI, 0.30–0.91) compared with conventional oxygen therapy [59]. However, compared with NIV, HFNC is not superior to NIV with regard to the rates of reintubation or post-extubation respiratory failure.
Postoperative Respiratory Failure
Postoperative respiratory failure accounts for more than 20% of all patients receiving ventilatory support [60,61]. Respiratory failure requiring unplanned reintubation in the postoperative period is associated with high morbidity, leading to a longer hospital stay and an increase in 30-day mortality [62-64]. The risk of reintubation was greatest within the first 6 hours after primary extubation, with consequences such as pneumonia (including aspiration), pulmonary edema, atelectasis, airway obstruction, and impaired brain function.
Generally, moderate evidence favors NIV as a technique for the prevention of reintubation in this situation [65]. Consequently, randomized trials evaluating the efficacy of HFNC are lacking; thus, HFNC is not typically used as a first-line therapy to prevent or manage postoperative respiratory failure. That said, it may be a reasonable alternative, particularly for patients who do not tolerate NIV well.
Hernández et al. [57] reported that the immediate application of HFNC was associated with a lower risk of respiratory failure and reintubation at 72 hours when compared with conventional oxygen therapy. In a study by Corley et al. [66], 155 obese patients (body mass index 30 kg/m2) undergoing cardiopulmonary bypass surgery were assigned to either the HFNC group (35–50 L/min) or the nasal cannula or face mask group (2–6 L/min) for 8 hours post-extubation. The groups were similar with regard to oxygenation, dyspnea, and the radiographic features of atelectasis. In another study, Yu et al. [67] compared HFNC with conventional oxygen treatment after thoracoscopic lobectomy. A total of 110 patients at moderate to high risk of reintubation were randomized postoperatively to receive either HFNC (35–60 L/min) or low-flow oxygen administered via nasal cannula or face mask. HFNC treatment was associated with a lower rate of hypoxemia (12% vs. 29%) and a decreased need for NIV (4% vs. 17%). Among the participants receiving conventional oxygen therapy, five reintubations were required, compared with none in the HFNC group.
In a study comparing HFNC with NIV, 830 patients who either developed or were at risk of developing acute respiratory failure after cardiothoracic surgery were randomly assigned to receive either HFNC or NIV. The HFNC treatment was conducted at 50 L/min and an FiO2 of 50%, whereas NIV involved bilevel positive airway pressure for at least 4 hours each day (pressure support, 8 cm H2O; PEEP, 4 cm H2O) [68]. No statistically significant differences were observed between the HFNC and NIV groups in treatment failure rate (reintubation, switch to the other treatment, or treatment discontinuation; HFNC 21% and NIV 22%). Similarly, the mortality rates were not statistically different (7% and 6%, respectively). However, skin breakdown, as expected, was more commonly encountered with NIV (10% vs. 3%).
In a meta-analysis of seven randomized trials involving 2,781 patients, HFNC was associated with a similar reintubation rate to both conventional oxygen therapy (RR, 0.58; 95% CI, 0.21–1.60) and NIV (RR, 1.11; 95% CI, 0.88–1.40) [69]. However, in a subgroup analysis of critically-ill patients, the HFNC group exhibited a lower reintubation rate than the conventional oxygen therapy group (RR, 0.35; 95% CI, 0.19–0.64).
In another meta-analysis of 14 studies, HFNC was associated with a statistically insignificant reduction in intubation rate and a reduction in length of hospital stay [70]. In contrast, in a subsequent meta-analysis of 9 trials, compared with conventional oxygen therapy, the use of HFNC postoperatively lowered reintubation rates (RR, 0.32; 95% CI, 0.12–0.88) and decreased the need to escalate respiratory support (e.g., switching to NIV; RR, 0.54; 95% CI, 0.31–0.94) [59]. However, HFNC had no effect on mortality rate, length of ICU or hospital stay, or rate of postoperative hypoxia.
Acute Hypoxemic Respiratory Failure in Immunosuppressed Patients
The mortality rate is relatively high among immunosuppressed patients with acute respiratory failure who need mechanical ventilation [71]. In this situation, NIV is recommended as first-line therapy, and it has been found to be effective in relieving sensations of dyspnea. In two studies, results have indicated that NIV is associated with less frequent intubations and lower mortality relative to conventional oxygen therapy [72].
A post hoc examination of the FLORALI study [27] indicated that among immunosuppressed patients, NIV was associated with more frequent intubation and a higher mortality rate than conventional oxygen therapy or HFNC [23]. A retrospective study of patients with cancer suggested that HFNC treatment was associated with a lower 28-day mortality rate than treatment with conventional oxygen therapy, NIV, or both (35% in the HFNC group vs. 57% in the non-HFNC group) [73]. When HFNC was compared with NIV as first-line therapy in a prospective observational study, it was found to be associated with reduced frequency of intubation (35% vs. 55%, respectively) and reduced mortality (20% vs. 40%, respectively) [74]. Notably, however, HFNC was not effective as a rescue treatment after the failure of conventional oxygen therapy or NIV [24], indicating that HFNC is best suited for early application.
Additionally, HFNC has been observed to reduce the rate of respiration and dyspnea in immunosuppressed patients, resembling its effects in patients who are not immunosuppressed [26,75-77]. Thus, HFNC may be a more easily tolerated alternative device that can provide adequate oxygenation and effective palliation, even for those immunosuppressed, “do not intubate” patients.
Acute Hypoxemic Respiratory Failure in COVID-19
When the oxygen requirement or work of breathing is increased, treatment options are HFNC, an NIV device, or invasive mechanical ventilation after intubation. Generally, clinical physicians favor noninvasive modalities (HFNC or NIV) over invasive mechanical ventilation.
While one retrospective study reported reduced rates of intubation and mechanical ventilation with HFNC [78], another retrospective study including noninvasive modalities reported no differences in the intubation rate for patients for coronavirus disease 2019 (COVID-19) treated with HFNC (29%), continuous positive airway pressure (25%), or other modes of NIV (28%) [79]. Additionally, no differences in mortality were observed.
Grieco et al. [80] compared helmet NIV and HFNC in 110 individuals with moderate to severe acute hypoxemic respiratory failure due to COVID-19. No significant difference was observed in days free of respiratory support at the 28-day mark (helmet NIV, 20 days; HFNC, 18 days). However, patients receiving helmet NIV had lower rates of intubation (30% vs. 51%) and experienced more days free of invasive mechanical ventilation (28 vs. 25 days).
HFNC is an aerosol-generating procedure that can potentially increase the risk of viral transmission. In spontaneously breathing patients with suspected or documented COVID-19, when HFNC is used, airborne in addition to standard precautions should be undertaken (i.e., full personal protective equipment; placing a surgical mask on the patient during HFNC when health care workers are in the room or the patient is being transported, or starting at the lowest effective flow rate).
CONTRAINDICATIONS
No randomized clinical trials have reported contraindications of HFNC as a primary endpoint. As such, no absolute contraindications have been identified. Relative contraindications to HFNC include any factor that prevents a nasal cannula from being appropriately fitted, such as irregularities of the nose, face, or airway or a history of surgery of those regions. Some experts avoid HFNC following upper airway surgery to avoid the theoretical risk that the high pressure may precipitate venous thromboembolism.
CONCLUSIONS
The HFNC is a method of respiratory support in which a high flow of humidified and heated oxygen is delivered at a set concentration via a unique device. HFNC is being increasingly used for patients with respiratory failure of diverse etiologies.
The advantages of HFNC over conventional oxygen systems or NIV include improved comfort, the facilitation of expectoration due to greater humidification of secretions, the washout of upper respiratory dead space to improve ventilation efficiency, a small positive airway pressure effect, and high flow rates to minimize the entrainment of room air for reliable delivery of FiO2.
HFNC has been successfully used in several settings such as severe acute respiratory failure, extubation failure, peri-intubation, postoperative respiratory failure, and others. However, the indications are not absolute, with much of the proven benefit subjective and physiologic. The choice of oxygen delivery system should be patient-specific, and factors to consider include institutional availability, clinicians’ judgment, patients’ preferences, the level of necessity for ventilation and PEEP, and hypoxemic severity.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This paper was supported by the fund of the Biomedical Research Institute at Jeonbuk National University Hospital. Jeonbuk National University Hospital played no role in the design of this study; collection, analysis, and interpretation of data; or writing of the manuscript.