In-hospital mortality prediction using frailty scale and severity score in elderly patients with severe COVID-19
Article information

Abstract
Background
Elderly patients with coronavirus disease 2019 (COVID-19) have a high disease severity and mortality. However, the use of the frailty scale and severity score to predict in-hospital mortality in the elderly is not well established. Therefore, in this study, we investigated the use of these scores in COVID-19 cases in the elderly.
Methods
This multicenter retrospective study included severe COVID-19 patients admitted to seven hospitals in Korea from February 2020 to February 2021. We evaluated patients’ Acute Physiology and Chronic Health Evaluation (APACHE) II score; confusion, urea nitrogen, respiratory rate, blood pressure, 65 years of age and older (CURB-65) score; modified early warning score (MEWS); Sequential Organ Failure Assessment (SOFA) score; clinical frailty scale (CFS) score; and Charlson comorbidity index (CCI). We evaluated the predictive value using receiver operating characteristic (ROC) curve analysis.
Results
The study included 318 elderly patients with severe COVID-19 of whom 237 (74.5%) were survivors and 81 (25.5%) were non-survivors. The non-survivor group was older and had more comorbidities than the survivor group. The CFS, CCI, APACHE II, SOFA, CURB-65, and MEWS scores were higher in the non-survivor group than in the survivor group. When analyzed using the ROC curve, SOFA score showed the best performance in predicting the prognosis of elderly patients (area under the curve=0.766, P<0.001). CFS and SOFA scores were associated with in-hospital mortality in the multivariate analysis.
Conclusions
The SOFA score is an efficient tool for assessing in-hospital mortality in elderly patients with severe COVID-19.
INTRODUCTION
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was first identified in Wuhan, China in December, 2019. SARS-CoV-2 causes coronavirus disease 2019 (COVID-19). The World Health Organization declared COVID-19 to be a pandemic in March, 2020 [1]. In the Korea, there have been 551,551 cases diagnosed with COVID-19 and 4,591 deaths from January 3, 2020, to December 17, 2021. As of December 12, 2021, 83,142,509 vaccine doses were administered. Vaccination is currently being implemented worldwide to prevent COVID-19 [2-4]; however, vaccination has not completely prevented COVID-19 [5]. With the recent increase in the number of patients with COVID-19, Korea is suffering from a rapid increase in the number of severely ill patients and a shortage of intensive care unit beds.
Elderly people have a higher COVID-19 severity and mortality than younger people [6-9]. In addition, elderly patients with COVID-19 have more underlying diseases and higher frailty at admission than younger patients [10-14]. High severity score and high frailty score are expected to assist in predicting mortality rate of elderly patients hospitalized with COVID-19 [15-18]. However, it is not well-known whether the best assessment for predicting in-hospital mortality is bassline frailty or the COVID-19 severity score. Therefore, in this study, we aimed to investigate whether the frailty scale and the currently used severity scoring system can predict in-hospital mortality in elderly patients with severe COVID-19.
MATERIALS AND METHODS
This multicenter retrospective study involved seven hospitals treating patients with severe COVID-19 in Korea from February 2, 2020 to February 28, 2021. We analyzed data collected from all hospitalized severe COVID-19 patients from the seven hospitals. The research was approved by the Ethical Committee of the Promoting Center (No. 2021-04-053) and local ethics committees. The need for written informed consent was waived due to the retrospective nature of the study.
All data were retrieved from electronic medical records. Information about patient characteristics, including gender, age, symptoms, and initial laboratory and radiologic findings, was collected. Moreover, data on the need for invasive treatment (mechanical ventilation, vasopressor treatment, and continuous renal replacement therapy [CRRT]), in-hospital mortality, and duration of hospital stay were extracted. The initial Acute Physiology and Chronic Health Evaluation (APACHE) II; Sequential Organ Failure Assessment (SOFA) score; confusion, urea nitrogen, respiratory rate, blood pressure, 65 years of age and older (CURB-65) score; modified early warning score (MEWS) and Charlson comorbidity index (CCI) score were analyzed to evaluate the patients’ condition at the time of admission. The clinical frailty scale (CFS) was used to indicate the patient's previous functional independence before hospitalization based on the patient’s medical status [19]. SARS-CoV-2 infection in hospitalized patients was confirmed via reverse transcriptase-polymerase chain reaction. Severe COVID-19 infection was defined as an oxygen saturation level of 94% or less in room air or a need for oxygen support [20]. These have been confirmed as indicators of COVID-19 severity.
Statistical Analysis
All data are expressed as the percentage for categorical variables and as the median and interquartile range for continuous variables. Pearson’s chi-square test or Fisher’s exact test was used for categorical data, and Student t-test or Mann-Whitney U-test was used for continuous data. Receiver operating characteristic (ROC) curve analysis was performed to evaluate prediction accuracy. The optimal cutoff value was chosen as the highest product of sensitivity and specificity. Cox regression analysis was performed to identify the predictors of in-hospital mortality. All P-values were two-tailed with statistical significance set at P<0.05. No imputation strategy was conducted because cases of missing data were rare (90/17,718, 0.5%). There were no missing values for frailty scale and severity scores. We used the IBM SPSS ver. 22.0 (IBM Corp., Armonk, NY, USA) to perform all statistical analyses.
RESULTS
Patients’ Baseline Characteristics
Of the 1,565 hospitalized COVID-19 patients, 318 patients ≥65 years old with severe COVID-19 were included. Of these, 237 patients (74.5%) comprised the survivor group and 81 (25.5%) comprised the non-survivor group (Figure 1).
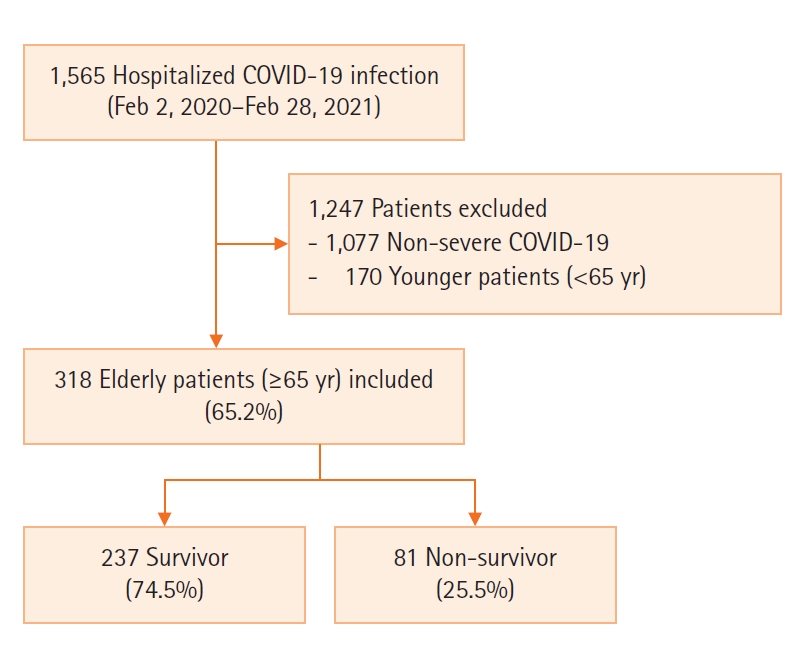
Flowchart of patients. COVID-19: coronavirus disease 2019.
Baseline patient characteristics at the time of admission are presented in the Table 1. The median ages of the survivor and non-survivor groups were 76 years (interquartile range [IQR], 69–84) and 80 years (IQR, 75–85), respectively. Chronic obstructive pulmonary disease (COPD; 8.6% vs. 2.1%, P=0.008) and diabetes mellitus (DM; 50.6% vs. 31.6%, P=0.002) were more common in the non-survivor group than in the survivor group. The non-survivor group had a lower diastolic blood pressure (67 mm Hg [53–79] vs. 72 mm Hg [64–82], P=0.002), Glasgow coma scale (15 [12–15] vs. 15 [15–15], P<0.001), and higher respiratory rate (RR; 22/min [20–26] vs. 20/min [19–22], P=0.003) than the survivor group. The non-survivor group patients had higher initial white blood cell (WBC) counts; neutrophil-to-lymphocyte ratios (NLRs); and blood urea nitrogen (BUN), creatinine, and C-reactive protein levels than survivor group patients. Non-survivor group patients also had lower initial hemoglobin levels, platelet counts, and albumin levels. Normal initial radiographs were fewer in the non-survivor group than in the survivor group (8.6% vs. 18.6%, P=0.036).
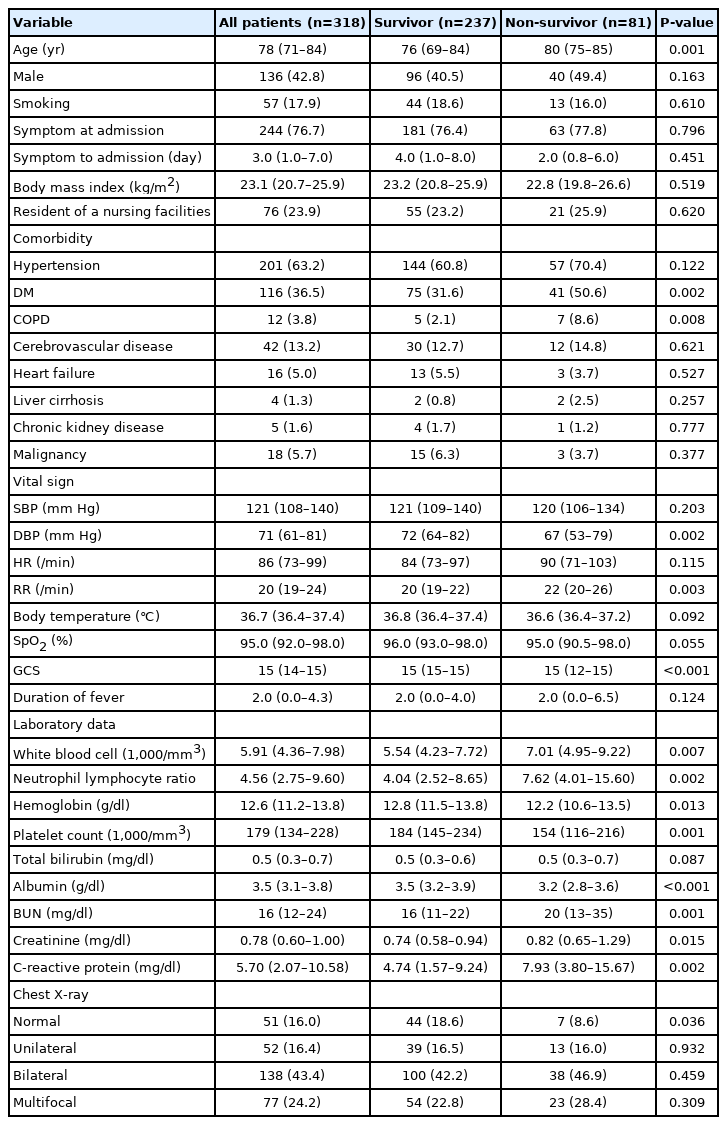
Baseline characteristics of elderly patients with severe COVID-19 at the time of admission
Treatment and Clinical Outcomes between Survivor and Non-survivor Groups
The treatment and outcomes of patients are presented in Table 2. The use of antibiotics (77.8% vs. 62.4%, P=0.012), vasopressors (38.3% vs. 7.2%, P<0.001), CRRT (19.8% vs. 1.7%, P<0.001), and steroids (90.1% vs. 72.2%, P=0.001) was higher in the non-survivor group than in the survivor group. Extracorporeal membrane oxygenation (ECMO; 8.6% vs. 1.3%, P<0.001), invasive mechanical ventilation (54.3% vs. 15.2%, P<0.001), and high-flow nasal cannula (59.3% vs. 26.2%, P<0.001) were more commonly used in the non-survivor group. Compared with the survivor group, the non-survivor group had a higher proportion of patients with do-not-resuscitate (DNR) orders (72.8% vs. 7.2%, P<0.001).
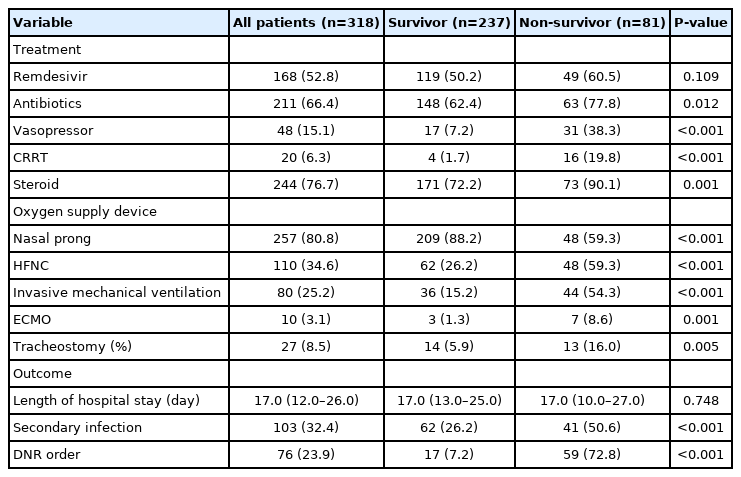
Treatment and clinical outcomes of elderly patients with severe COVID-19
Frailty Scale and Severity Scores between the Survivor and Non-survivor Groups
Table 3 shows the frailty and severity scores of elderly patients. Compared with the survivor group, the non-survivor group had higher CFS and CCI. In addition, the APACHE II, SOFA, CURB-65 scores, and MEWS were higher in the non-survivor group than in the survivor group.

Frailty scale and severity score of elderly patients with severe COVID-19
Prognostic Value of the Frailty Scale and Severity Score
The performance of the CFS, CCI, APACHE II, SOFA, CURB-65, and MEWS in predicting in-hospital mortality was evaluated using ROC curves (Figure 2). The SOFA score demonstrated the best performance in predicting the prognosis of elderly severe COVID-19 patients (area under the curve [AUC], 0.766; P<0.001). The CFS (AUC, 0.692; P<0.001), CCI (AUC, 0.652; P<0.001), APACHE II score (AUC, 0.699; P<0.001), CURB-65 (AUC, 0.672; P<.001), and MEWS (AUC, 0.646; P<0.001) demonstrated poor performance. The prognostic cut-off value of the SOFA score was 2.50 (sensitivity, 72.8%; specificity, 70.5%).
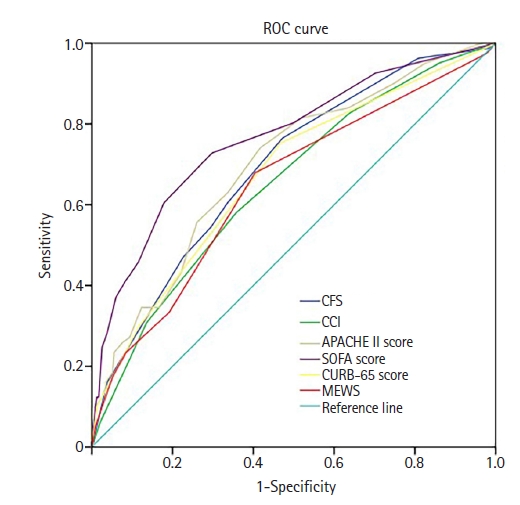
Receiver operating characteristic (ROC) curves of the clinical frailty scale (CFS), Charlson comorbidity index (CCI), Acute Physiology and Chronic Health Evaluation (APACHE) II, Sequential Organ Failure Assessment (SOFA), confusion, urea nitrogen, respiratory rate, blood pressure, 65 years of age and older (CURB-65) scores, and modified early warning score (MEWS) in predicting patients’ in-hospital mortality.
Predictors of Patients’ In-hospital Mortality
Table 4 shows the risk factors associated with in-hospital mortality. In multivariate analysis, age (odds ratio [OR], 1.029; 95% confidence interval [CI], 0.999–1.059; P=0.054), high CFS (OR, 1.274; 95% CI, 1.112–1.460; P<0.001), high SOFA score (OR, 1.144; 95% CI, 1.082–1.211; P<0.001), DM (OR, 1.988; 95% CI, 1.240–3.188; P=0.001), COPD (OR, 2.462; 95% CI, 1.093–5.546; P=0.030), and high WBC count (OR, 1.051; 95% CI, 1.003–1.101; P=0.038) were shown to be factors associated with in-hospital mortality.
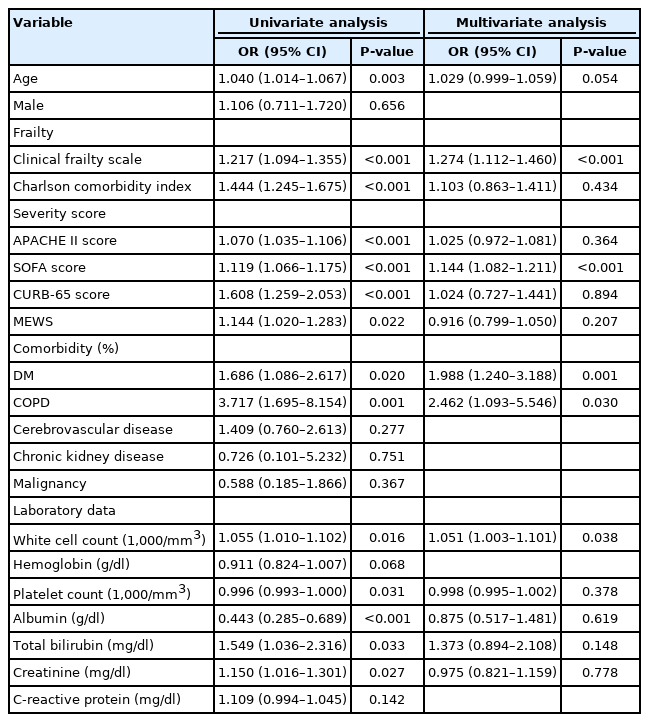
Univariate and multivariate risk factors associated with in hospital mortality (Cox regression model)
DISCUSSION
In this study, the in-hospital mortality rate of elderly patients with severe COVID-19 was 25.5%. Non-survivor group were older, had more underlying comorbidities, frailer, and more severe by severity scores than the survivor group. SOFA score was the best predictor of in-hospital mortality. High CFS, high SOFA score, age, a concurrent diagnosis of COPD, a concurrent diagnosis of DM, and high WBC count were risk factors for in-hospital mortality in the elderly patients with severe COVID-19.
Elderly patients commonly have underlying diseases such as DM and COPD. Additionally, the non-survivor group patients frequently required treatments such as invasive mechanical ventilation, CRRT, and ECMO. These patients also had DNR orders more frequently. The required treatment and DNR order findings are consistent with those of previous studies [21-26]. In Gao et al.’s study [26], which included older (≥65 years) COVID-19 patients, the deceased group had more morbidities including cardiovascular diseases (49% vs. 20%, P<0.001), respiratory diseases (51% vs. 11%, P<0.001), chronic kidney disease (29% vs. 5%, P<0.001) and cerebrovascular disease (20% vs. 3%) than the discharged group. In a study by Vrillon et al. [21], included the very elderly (≥85 years) COVID-19 patients, the non-survivor group had more cardioneurovascular diseases (68.2% vs. 37.0%, P=0.013), more complications like acute respiratory distress syndrome (95.5% vs. 1.9%, P<0.001), and needed more frequent treatment with oxygen (95.5% vs. 46.3%, P<0.001) compared with the survivor group.
In this study, the non-survivor group had higher WBC counts and NLR, BUN, creatinine, and C-reactive protein levels than the survivor group. The non-survivor group also had lower hemoglobin levels, platelet counts, and albumin levels than survivor group. In a study of elderly patients with COVID-19 by Gao et al. [26], the deceased group subjects showed significantly higher levels of C-reactive protein and BUN and significantly lower lymphocyte counts than the discharged group subjects. Li et al.’s study [27], in the elderly (≥60 years) patients with COVID-19, showed that higher WBC and neutrophil counts, creatine kinase-MB levels, D-dimer levels, and procalcitonin levels and lower albumin levels, lower pH values, presence of hypercapnia, and presence of hypoxia were associated with higher mortality. The results of these studies were similar to those of our study that was focused on elderly patients with severe COVID-19.
Elderly patients with severe COVID-19 were frailer and had higher disease severity. Pranata et al. [16] showed that a 12% increase in patient mortality was associated with a one point increase in CFS and that CFS was associated with mortality in a linear fashion. In a study of older patients with COVID-19 by Darren et al. [15], the mortality rate was higher in the patients who had a CFS score of 6 or higher than in the patients with CFS of 1–3. In a study by Tuty Kuswardhani et al. [28], compared to patients with a CCI score of 0, patients with a CCI score of 1–2 and ≥3 had higher mortality and poorer outcome. Additionally, the higher the SOFA score, the higher was the mortality rate in patients with severe COVID-19. In this study, the prognostic cut-off value of the SOFA score for in-hospital mortality was 2.50. In Yang's study [18], the cut-off SOFA score value for predicting severe COVID-19 was 2, and the cut-off value for predicting mortality was 5. In a study of patients with suspected infection admitted to an intensive care unit, an increase in SOFA score of 2 or more was associated with in-hospital mortality [17]. In our study, the SOFA score cut-off of 2.5 seems lower than the SOFA score of critically ill ICU patients in general. This is probably due to the effect of respiratory failure being the main cause of exacerbation in many patients with severe COVID-19. While there have been studies on the usefulness of each score for predicting severity and mortality, no study has analyzed an overall frailty scale and severity score. In this study, scores indicating frailty and patient severity were analyzed, and the SOFA score showed the best predictive power for mortality. However, with the current ICU bed shortage situation, considering several factors when determining ICU admission is preferred [29-31]. Therefore, in actual practice, considering several factors related to mortality, such as CFS, in addition to the SOFA score is necessary in ICU triage.
Age, high CFS, high SOFA score, comorbidities such as DM, COPD, and high WBC count were risk factors of in-hospital mortality in this study. These risk factors have also been shown in other studies. Frailty is related to the prognosis of elderly patients. A multicenter study of elderly COVID-19 patients ≥70 years old showed that higher frailty was associated with higher 30-day mortality and a higher rate of treatment limitation [32]. Pranata et al. [16] and Aliberti et al. [33] also showed that higher clinical frailty scores were associated with higher mortality. In other studies, factors associated with mortality include age; Charlson index; presence of diabetes, COPD, CKD, hypertension, or dementia; high d-dimer level; and high neutrophil-lymphocyte ratio [34-36].
This study has several limitations. First, the frailty scale and severity scores were calculated by reviewing medical records and collecting clinical data from an electronic record database. While these scores may differ from actual scores, the difference was judged to be negligible. Second, the hospital participating in the study is a hospital that treats severe COVID-19 patients; patients who have been transferred from the living center and other hospitals may initially show higher severity and poorer laboratory data. However, since most hospitals that treat critically ill patients have many patients from other hospitals, the evaluation and results shown in this study are still useful.
In conclusion, the in-hospital mortality rates of elderly patients with severe COVID-19 was 25.5%. The SOFA score showed the best predictive performance, and the prognostic cut-off value was 2.50. The SOFA score was the most useful tool for predicting critical care and in-hospital mortality in elderly patients with severe COVID-19; and other factors associated with in-hospital mortality were age, CFS, concurrent diagnosis of DM or COPD, and high WBC count.
Key Message
▪ The in-hospital mortality of elderly patients with severe coronavirus disease 2019 (COVID-19) was 25.5%.
▪ The non-survivor group had more underlying diseases, and their initial frailty scale and severity scores tended to be higher than those in the survivor group.
▪ The Sequential Organ Failure Assessment (SOFA) score demonstrated the best performance in predicting the in-hospital mortality of elderly patients with severe COVID-19.
▪ Clinical frailty scale and SOFA scores were associated with in-hospital mortality in multivariate analyses, and these may assist in treatment decision-making.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: YSN, JHK, SIL. Data curation: all authors. Formal analysis: SIL. Methodology: SIL. Visualization: YSN, JHK, SIL. Writing–original draft: all authors. Writing–review & editing: all authors.