Relationship between positive end-expiratory pressure levels, central venous pressure, systemic inflammation and acute renal failure in critically ill ventilated COVID-19 patients: a monocenter retrospective study in France
Article information

Abstract
Background
The role of positive pressure ventilation, central venous pressure (CVP) and inflammation on the occurrence of acute kidney injury (AKI) have been poorly described in mechanically ventilated patient secondary to coronavirus disease 2019 (COVID-19).
Methods
This was a monocenter retrospective cohort study of consecutive ventilated COVID-19 patients admitted in a French surgical intensive care unit between March 2020 and July 2020. Worsening renal function (WRF) was defined as development of a new AKI or a persistent AKI during the 5 days after mechanical ventilation initiation. We studied the association between WRF and ventilatory parameters including positive end-expiratory pressure (PEEP), CVP, and leukocytes count.
Results
Fifty-seven patients were included, 12 (21%) presented WRF. Daily PEEP, 5 days mean PEEP and daily CVP values were not associated with occurrence of WRF. 5 days mean CVP was higher in the WRF group compared to patients without WRF (median [IQR], 12 mm Hg [11-13] vs. 10 mm Hg [9–12]; P=0.03). Multivariate models with adjustment on leukocytes and Simplified Acute Physiology Score (SAPS) II confirmed the association between CVP value and risk of WRF (odd ratio, 1.97; 95% confidence interval, 1.12–4.33). Leukocytes count was also associated with occurrence of WRF in the WRF group (14 G/L [11–18]) and the no-WRF group (9 G/L [8–11]) (P=0.002).
Conclusions
In mechanically ventilated COVID-19 patients, PEEP levels did not appear to influence occurrence of WRF. High CVP levels and leukocytes count are associated with risk of WRF.
INTRODUCTION
Acute kidney injury (AKI) is a frequent complication among patient hospitalized for coronavirus disease 2019 (COVID-19) [1], with a wide range of incidence reported since the beginning of the epidemic, from 0.5% [2] to 36.6% [3]. Recently, a systematic review estimated the incidence around 10% among patient hospitalized for COVID-19 [4]. In critically ill patients, the incidence of AKI has been reported between 26% and 56% [4-6] and may be associated with severe complications such as the use of renal replacement therapy [7], progression of chronic kidney disease [8], and a higher rate of hospital mortality [9,10].
Pathophysiology of AKI in patients hospitalized in intensive care unit (ICU) for COVID 19 acute respiratory distress syndrome (ARDS) is multifactorial. Virus may exert a direct role on the renal parenchyma, by infecting the cells that express angiotensin-converting enzyme 2 (ACE-2) receptors [11] (podocytes and proximal tubular cells [12]). Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) causes an increase in ACE activity and an overproduction of angiotensin II, leading to a proinflammatory state damaging the kidney [13]. It can also have an effect on glomerular cells [14], with collapsing glomerulopathy [15]. In addition, COVID-19 can lead to elevated levels of inflammatory cytokines, which can cause endothelial dysfunction, microvascular thrombosis and tubular cells damages [16]. Besides, hemodynamic consequences of ventilatory support (i.e., mechanical ventilation with positive pressure) could also directly impact glomerular function. Positive pressure ventilation has been shown to decreases renal blood flow, glomerular filtration rate, urine output, excretion of creatinine and sodium [17,18]. Previous studies has shown that elevated central venous pressure (CVP) is associated with AKI occurrence in ICU, especially in septic shock patients [19,20], suggesting a crucial role of the venous congestion in the development of AKI. By increasing intra thoracic and CVP, positive end-expiratory pressure (PEEP) level could have a direct impact on renal perfusion and occurrence of AKI [21].
The objective of the study was to investigate the relationship between hemodynamics, ventilatory parameters and systemic inflammation, and the progression of AKI in COVID-19 patients who required mechanical ventilation.
MATERIALS AND METHODS
Study Design
We conducted a single center, retrospective cohort study in a 43 beds ICU in France during the COVID-19 surge. This study was approved by Institutional Review Board of Paris 7 University (No. 00006477, HUPNVS). Informed consent was waived by the board.
Patient Population
All patients admitted in ICU from March 2020 to July 2020 for a SARS-CoV-2 pneumoniae were screened. SARS-CoV-2 pneumoniae was defined by the association of evocative lung lesions seen in computed tomography scan or thoracic radiography and a positive polymerase chain reaction result for SARS-CoV-2. Patients were included if they were 18 years old or older and if they required mechanical ventilation for respiratory support during ICU stay. Patients were excluded if they were mechanically ventilated for another reason than respiratory failure, and if another diagnosis than SARS-CoV-2 was possible to explain the lung injury. Patients were also excluded if they had an AKI due to another disease than SARS-CoV-2 pneumoniae during the 3 days before admission to ICU.
Data Collection
Collected data were extracted from electronic and paper medical records. Day 1 was defined as the first day of mechanical ventilation. Demographic data included age, sex, comorbidities, treatment by renin angiotensin inhibitor, immunosuppressive therapy, use of corticosteroids, antiplatelet drug or anticoagulant therapy. Charlson comorbidity index, Simplified Acute Physiology Score (SAPS) II and Sequential Organ Failure Assessment (SOFA) scores [22,23] were calculated 24 hours after admission in ICU. Biological parameters included serum creatinine, urea, leukocytes count, neutrophils count, lymphocytes count, oxygen partial pressure in arterial blood.
Ventilatory and hemodynamic parameters included PEEP, plateau pressure, tidal volume, fraction of inspired oxygen and CVP and correspond to the mean values of the day (4–6 measurements every day for each parameter). According to local nursing monitoring protocols, plateau pressure reported in the medical records were the values of pressure displayed by the ventilator after a 5 seconds inspiratory pause. Criteria for ARDS were evaluated according to Berlin consensus [24]. Diuresis and daily fluid balance measured every day at the same hour were collected.
Patient Management
All patients were managed according to local protocol based on international guidelines. Respiratory management included limitation of tidal volume to 6 ml/kg, limitation of plateau and driving pressure, use of neuromuscular blockade and prone positioning session of at least 16 hours if necessary. PEEP levels were individualized according to a local protocol to improve oxygenation without deteriorating compliance and cardiac output. Patent foramen ovale and pleural effusions were systematically looked for and considered for drainage.
Hemodynamics optimizations were performed using cardiac output monitors for all patients, principally esophageal Doppler. Central line in the superior venous territory and arterial lines were inserted in all patients. CVP was measured continuously.
Definitions
The diagnosis of AKI was based on the Kidney Disease Improving Global Outcome (KDIGO) classification [25]. Severe AKI at admission was defined as an increase in serum creatinine level ≥2 times from baseline or ≥353.6 µmol/L or initiation of RRT corresponding to KDIGO stage 2 and 3. Baseline serum creatinine levels were measured in blood samples taken before hospital admission when available. When baseline creatinine was not available, the lowest serum creatinine level measured during the patient’s hospital stay was used if the glomerular filtration rate calculated with Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula was ≥75 mL/min/1.73m2. In other cases, the baseline creatinine level was estimated by using the modification of diet in renal disease equation with the assumption of an age-adjusted glomerular filtration rate because this approach performed best in terms of generating the smallest number of false negatives [26].
New, persistent and transient AKI
New severe AKI was defined as an increase in serum creatinine level ≥2 times from baseline or ≥353.6 µmol/L or initiation of RRT after 24 hours from inclusion in patients who had no severe AKI upon the initiation of mechanical ventilation (MV). Persistent severe AKI was defined as a steady or increase in KDIGO classification stage between the first 24 hours following initiation of MV and day 5 in patients with KDIGO stage ≥2 at inclusion or between the first 24 hours following initiation of MV and the last day of MV depending on which one comes first. Transient severe AKI was defined as a resolution or a downstaging of AKI between the first 24 hours following inclusion and day 5 (example from KDIGO stage 2 to KDIGO stage 1).
Worsening renal function
Worsening renal function (WRF) was defined as a new or persistent severe AKI (WRF+). Patients with no AKI or transient severe AKI were considered as patient without WRF (WRF–).
Primary endpoint
The primary endpoint of the study was to investigate the relationship between PEEP, CVP and WRF during the 5 days following the initiation of mechanical ventilation.
Secondary endpoints
The secondary endpoint was to identify other risk factors associated with WRF.
Statistical Analysis
Quantitative parameters are reported as median with interquartile range (IQR) and qualitative parameters are expressed as number and percentage. Categorical variables were compared using Fisher exact test as appropriate. Continuous variables were compared using Mann-Whitney U-test.
Actualized mean PEEP was defined by the cumulative mean PEEP dose, i.e., the mean PEEP between the day studied and the previous day. We also calculated mean values during 5 days for the daily PEEP, CVP, leukocytes count, and neutrophils count to reflect the overall exposition of the kidney, to elevated pressures and inflammation during the first days of mechanical ventilation.
We developed two multivariable models with adjustment for cofounding factors (SAPS II and mean leukocytes count for 5 days) to assess the association between mean CVP level for 5 days, mean PEEP level for 5 days and the risk of WRF. Predicted probabilities of WRF by the models were plotted together with significantly associated variables and a local polynomial regression fitting was performed to visually assess the relationship between the variable and the risk of WRF.
Finally, the relationship between PEEP level and CVP was explored using linear regression. A P-value lower than 0.05 has been considered significant. Odds ratio are reported with 95% confidence intervals (CIs). All statistical analyses were performed using R statistical software version 4.0.2 (R Core Team, 2020, R Foundation for Statistical Computing; https://www.R-project.org).
RESULTS
Baseline Characteristics
Seventy-three patients with SARS-CoV-2 pneumoniae were screened. Among them, 57 were mechanically ventilated and included in the study. All patients fulfilled Berlin criteria for ARDS. Flowchart is shown in Supplementary Figure 1.
Among the 57 included patients severe AKI was diagnosed in 16 patients (28%). Severe AKI was diagnosed at the time of intubation in 11 patients (19.3%). Among them, four patients presented a transient AKI, and seven patients had a persistent severe AKI. Forty-six patients (80.7%) had no severe AKI at the time of intubation, five developed a new severe AKI. Therefore, 12 patients were included in the WRF+ and 45 patients were included in the WRF– group.
Baseline characteristics are shown in Table 1. Patients in the WRF+ group were mainly females and had higher SOFA and SAPS II scores. They were more susceptible to have hypertension and a pre-existing chronic kidney failure. Leukocytes at admission were higher in the WRF+ group than in the WRF– group (median [IQR], 12 [11–14] vs. 9 [7–11]; P=0.01). Regarding the ventilatory parameters at day 1, there was no difference of ratio between the partial pressure in O2 and the inspiratory fraction of O2 (P/F ratio), PEEP, compliance, Pplat and inspiratory fraction of oxygen between groups. The CVP was also not different between groups at the time of intubation.
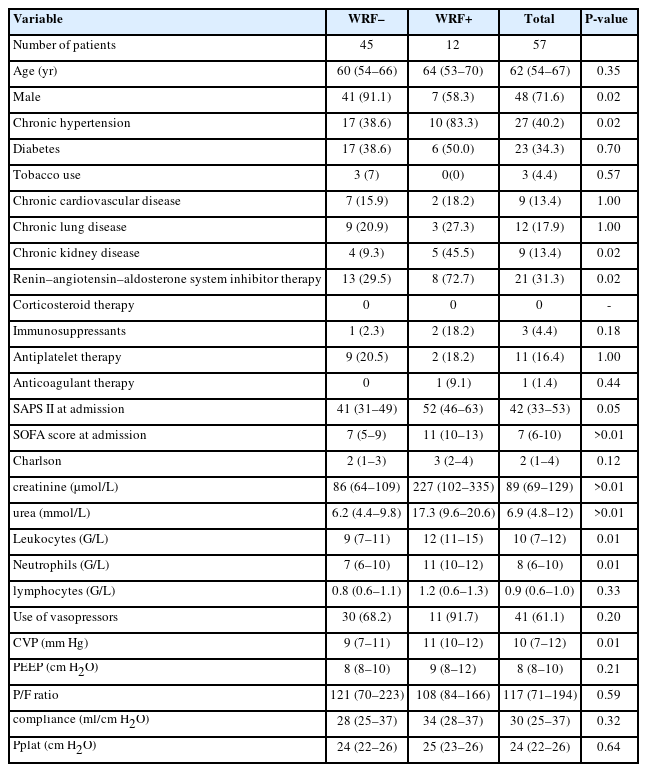
Demographic characteristics
Concerning the need for vasopressors, there was no difference in terms of the number of patients requiring vasopressors between the WRF– and WRF+ group (35 [81.4%] vs. 12 [100.0%], P=0.249). There was also no difference in terms of the vasopressors free days during the 5 days post intubation between the WRF– and WRF+ groups (median [IQR], 2 [0–4] vs. 1 [0–2]; P=0.13).
Association between AKI and Ventilatory Parameters
During the 5 days following the initiation of mechanical ventilation, there was no difference in daily compliance, daily PEEP and daily actualized mean PEEP between groups except for PEEP and actualized mean PEEP at day 2 (Figure 1, Supplementary Figures 2 and 3). The PEEP mean value during the 5 days was not different between the WRF+ and WRF–groups (median [IQR], 10 [9–11] vs. 8 [8–11]; P=0.09) (Table 2). The absence of association between PEEP and WRF persisted after multivariable analysis (Supplementary Table 1, Supplementary Figure 4).
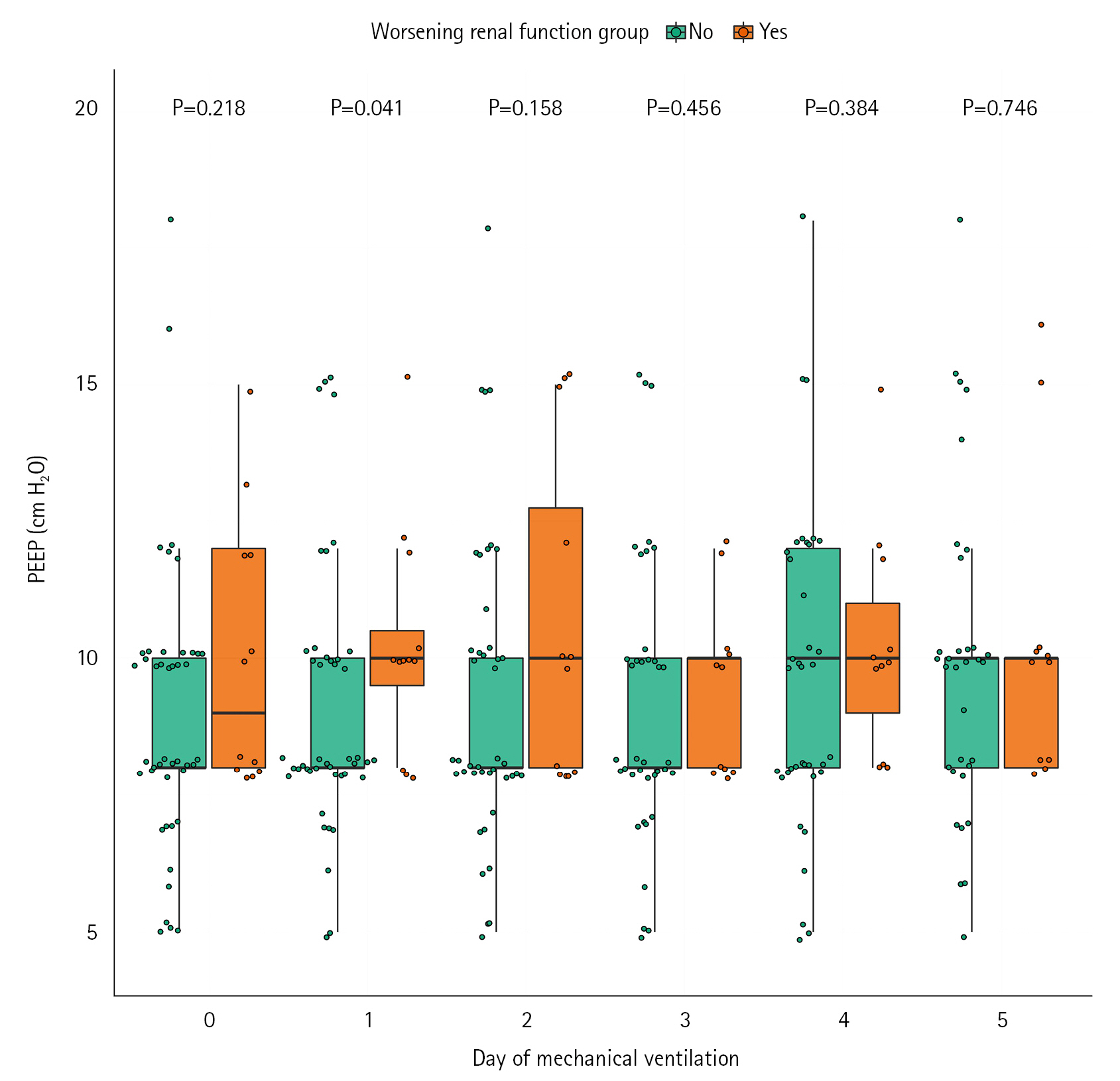
Comparison of daily positive end expiratory pressure (PEEP) during the 5 days following intubation.
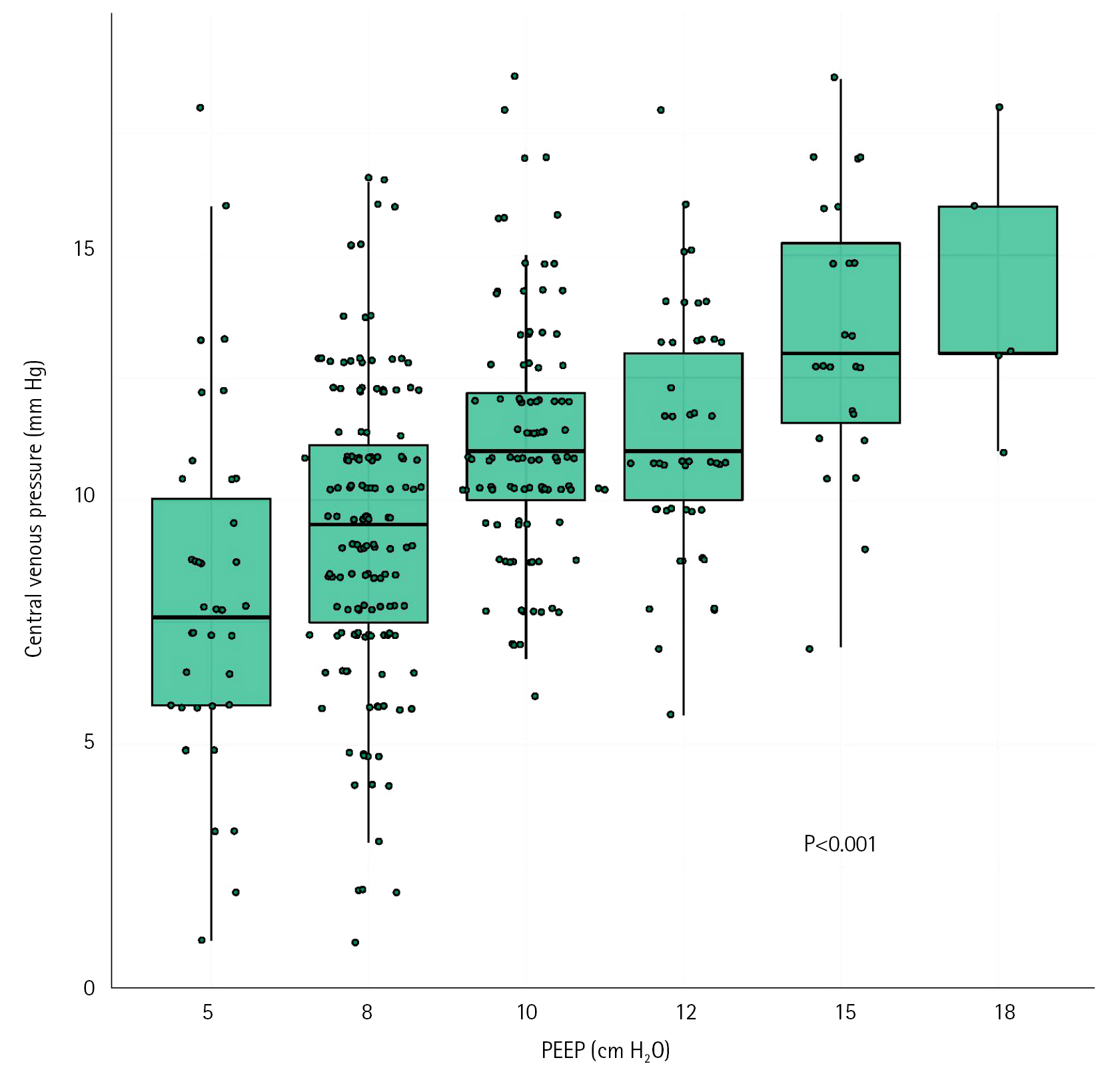
Relationship between central venous pressure and positive end expiratory pressure (PEEP).
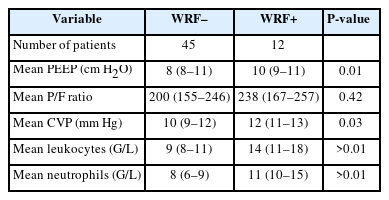
Mean values of PEEP, P/F ratio, CVP, leukocytes, and neutrophils during the 5 days following intubation
Association between Ventilatory Parameters, CVP and AKI
The daily values of CVP were not different between the two groups (Supplementary Figure 5). However, the mean value of CVP within 5 days after intubation was more elevated in the WRF+ group than in the WRF–group (median [IQR], 12 [11–13] vs. 10 [9–12]; P=0.03) (Table 2). Using multivariable analysis, there was a positive relationship between mean values of CVP during the 5 days and the risk of WRF, with an odd ratio for WRF of 1.97 (95% CI, 1.12–4.33) per increase of 1 mm Hg of CVP (Supplementary Table 2), and a significant increase in risk of WRF with CVP values above 10 mm Hg (Figure 2). Investigating the relationship between PEEP and venous pressure, there was a linear relationship between PEEP level and CVP (Figure 3).
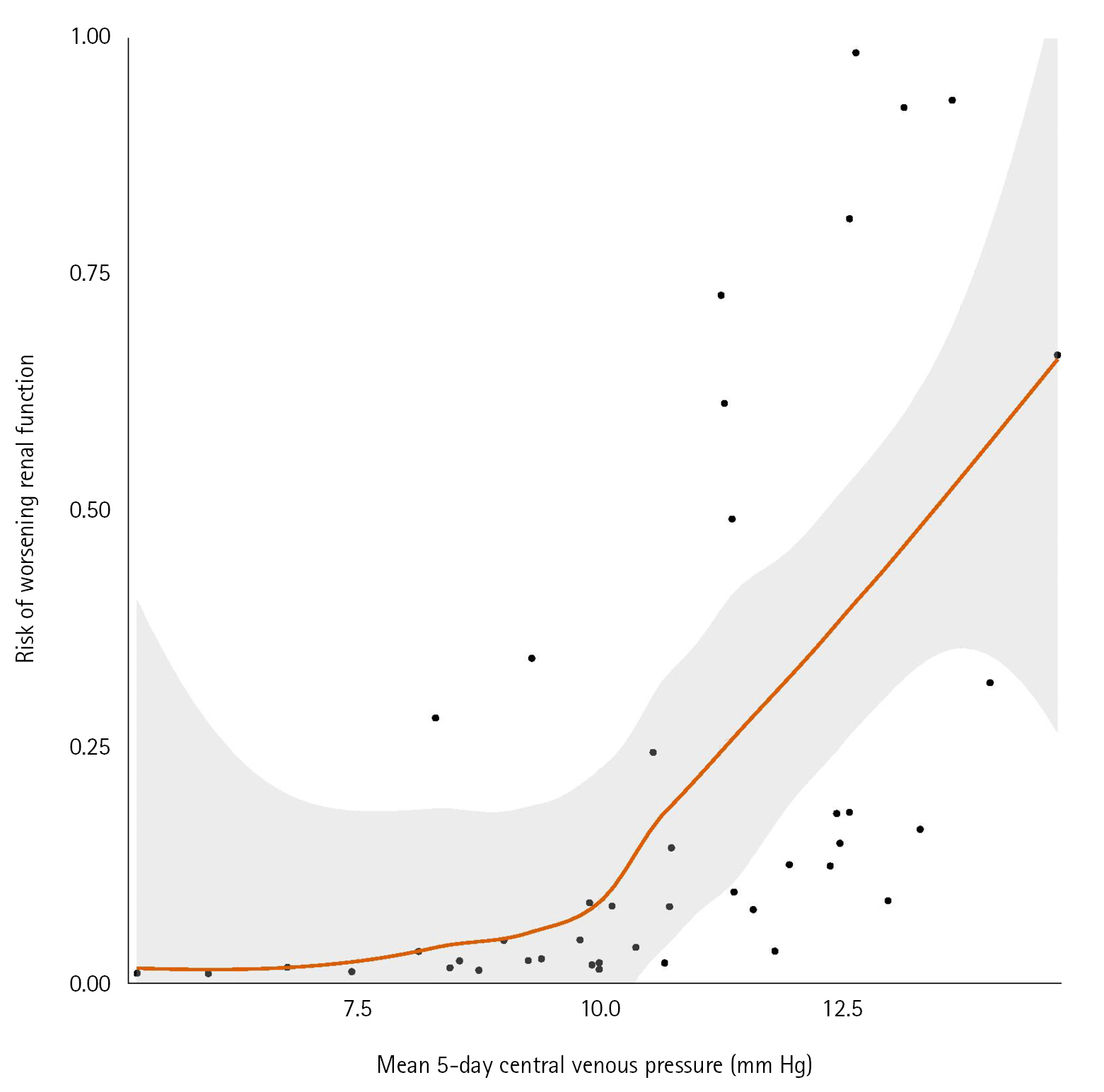
Risk of worsening renal function according to the mean value of central venous pressure during the 5 days.
Association between AKI and Biological Parameters
Daily leukocytes and neutrophils were more elevated in the WRF+ group (Figure 4, Supplementary Figure 6), except for neutrophils on the day 4. The mean value of leukocytes on the 5 days after intubation were 14 G/L (IQR, 11–18) in the WRF+ group and 9 G/L (IQR, 8–11) in the WRF– group (P=0.002), and mean value of neutrophils were also higher in the WRF+ group (11 G/L [IQR, 10–15]) than in the WRF– group (8 G/L [IQR, 6–9]) (P=0.001). We did not observe any difference in lymphocytes count between the two groups (Supplementary Figure 7).
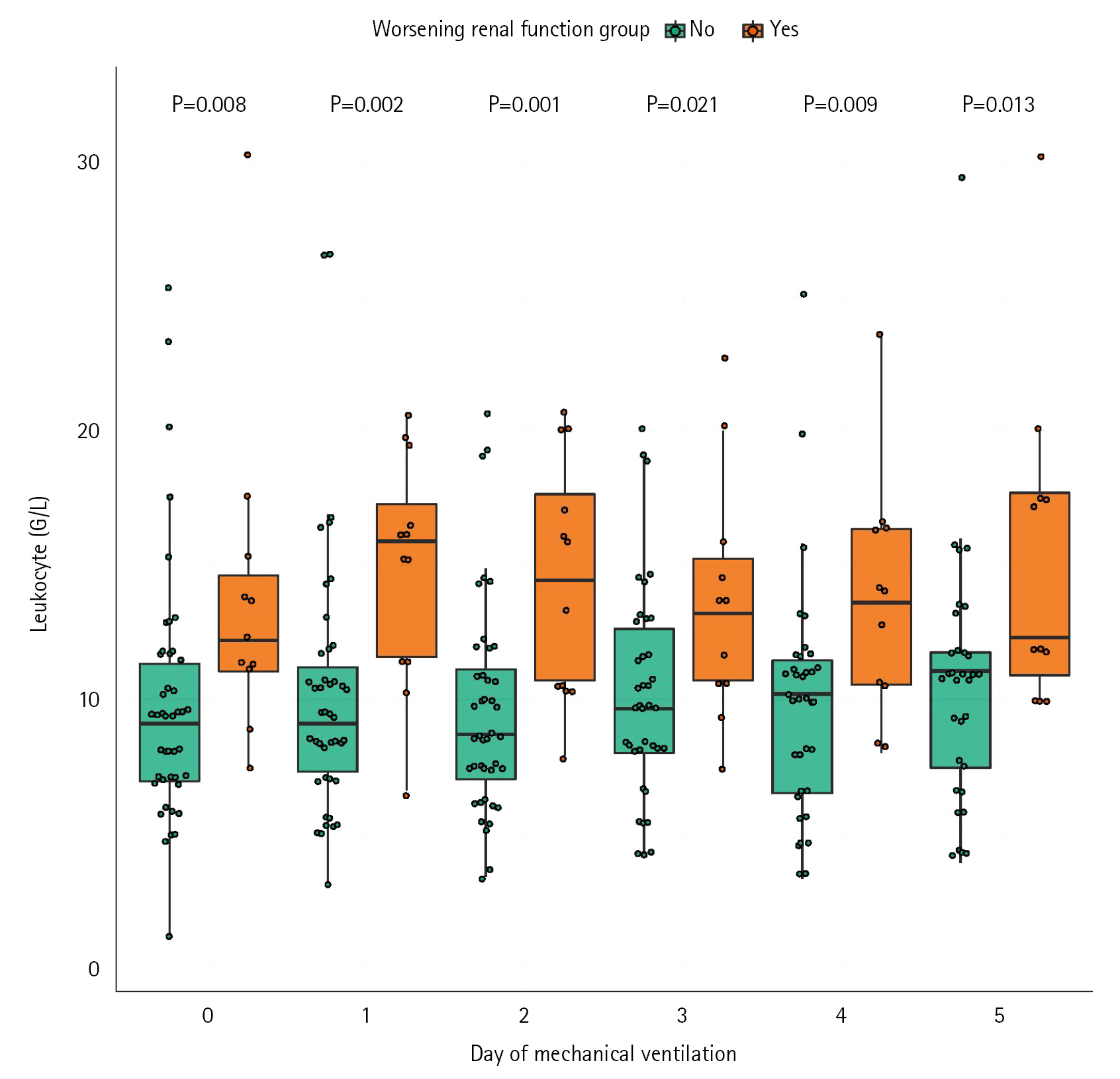
Comparison of daily leukocytes during the 5 days following intubation.
DISCUSSION
In the present study, we found no association between PEEP levels and WRF. CVP levels are associated with the risk of WRF, especially above 10 mm Hg. PEEP may be associated with WRF through its impact on CVP. Inflammation also seems to be a contributor to WRF. The relationship between PEEP and AKI has been evoked multiple times in the literature [27-30]. Anyway, few studies investigated the impact of PEEP levels on occurrence or persistence of AKI to date. The COVID-19 pandemic recently emphasized the major importance of adequate ventilator management of ARDS patients. We showed that PEEP has a dramatic impact on global hemodynamics and may reduce oxygen delivery while improving P/F ratio [31].
The contribution of right side pressure, i.e. CVP, to AKI has been well described [19,20]. A strength of our study is to investigate together PEEP and CVP impact on AKI. The global impact of PEEP on CVP is uncertain [32-34] and relies on various factors (hypovolemia, compliance, right heart function, etc.). It has been proven that PEEP increases CVP, although it is impossible to predict the raise in patients with altered lung compliance. It is therefore consistent with physiology and physiological studies to find an elevation of the PVC level with PEEP level. In our study, CVP levels increases with peep levels, but PEEP levels did not differ between patient with or without WRF. Consistently with literature [21], we found an increased risk of WRF with high values of CVP (above 10 mm Hg). These results highlight the fact that PEEP may contribute to occurrence of WRF through its impact on CVP. Therefore, ventilatory and hemodynamic management of COVID-19 ARDS patients should focus on the evolution of CVP in order to prevent kidney injury. Interestingly, we found that inflammation was a risk factor of WRF. One study has recently found that high neutrophils count in ICU was associated with severe AKI [35]. Our results support the hypothesis of a role of inflammation in case of AKI in COVID 19. Thus, management of the inflammatory part of AKI relies on the control of the disease and may respond to immunomodulatory treatments that were recently put under the light with the pandemic.
In the present study, we decided to consider both new AKI and persistent AKI together. This concept of WRF fits well with ICU daily practice. Indeed, a large proportion of AKI occurs before ICU admission [36]. It seems adequate to consider that the same factors contribute to both development and persistence of AKI.
Our study suffers several limitations. First, the retrospective, single center, nature of our study may prevent us generalizing our results. However, our center is expert in hemodynamic monitoring, with a trained and experienced team, implying that the CVP values reported can be considered reliable. More, all the patients were treated homogeneously, with local protocols in accordance with international guidelines [37].
Second, there were several imbalances between the two groups, and not every variables were taken into account in the analyses, likely due to the limited number of patients. Third, the CVP levels reported were relatively low. This can be explained by the fact that our teams is concerned about maintaining low CVP, in order to limit the repercussions of subsequent right side heart failure. Last, this study was conducted during the first wave of COVID 19, implying that none of these patients received immunomodulatory therapy such as dexamethasone or tocilizumab. In addition, some of these patients did not immediately benefit from enhanced preventive anticoagulation as recommended now [38].
Based on these results, it appears that kidney protection should be an objective of the ventilatory strategy. In mechanically ventilated COVID-19 patients, PEEP level did not appear to influence occurrence of WRF, high CVP levels and leukocytes count are associated with risk of WRF.
KEY MESSAGES
▪ In acute respiratory distress syndrome due to coronavirus disease 2019 (COVID-19), patients with high central venous pressure and high leucocytes count had a higher risk of acute kidney injury.
▪ Positive pressure expiratory levels did not appear to influence occurrence of acute kidney injury .
▪ These results suggest a major role of central venous pressure and inflammation on occurrence of acute kidney injury among patients ventilated for severe COVID-19.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING
None.
AUTHOR CONTRIBUTIONS
Conceptualization: PB, AM, BGC. Data curation: PB, BGC. Formal analysis: LM, BH. Methodology: EG, AM. Visualization: LM, RB, EG. Writing–original draft: PB, RB, NJ, MK, MC, BGC. Writing–review & editing: PB, BGC.
Acknowledgements
None.
SUPPLEMENTARY MATERIALS
Supplementary materials can be found via https://doi.org/10.4266/acc.2022.01494.
Multivariate model including 5 days mean PEEP, 5 days mean leukocytes and SAPS II for the prediction of worsening renal function
acc-2022-01494-Supplementary-Table-1.pdfMultivariate model including 5 days mean CVP, 5 days mean leukocytes and SAPS II for the risk of worsening renal function
acc-2022-01494-Supplementary-Table-2.pdfFlowchart. WRF: worsening renal function; COVID-19: coronavirus disease 2019; AKI: acute kidney injury.
acc-2022-01494-Supplementary-Fig-1.pdfComparison of daily actualized mean positive end expiratory pressure (PEEP) during the 5 days following intubation.
acc-2022-01494-Supplementary-Fig-2.pdfComparison of daily compliance during the 5 days following intubation.
acc-2022-01494-Supplementary-Fig-3.pdfRisk of worsening renal function according to the mean value of positive end expiratory pressure (PEEP) value.
acc-2022-01494-Supplementary-Fig-4.pdfComparison of daily central venous pressure during the 5 days following intubation.
acc-2022-01494-Supplementary-Fig-5.pdfComparison of daily neutrophils during the 5 days following intubation.
acc-2022-01494-Supplementary-Fig-6.pdfComparison of daily lymphocytes during the 5 days following intubation.
acc-2022-01494-Supplementary-Fig-7.pdf