
Articles
- Page Path
- HOME > Acute Crit Care > Volume 39(1); 2024 > Article
-
Original Article
Trauma Clinical characteristics and outcomes of obstetric patients transferred directly to intensive care units -
Saad Pirzada1
 , Kimberly Boswell2,3, Jerry Yang1, Samantha Asuncion1, Fernando Albelo1, Amanda Tuchler1, Lauren Becker4, Allison Lankford5, Emad Elsamadicy5, Quincy K Tran1,2,3
, Kimberly Boswell2,3, Jerry Yang1, Samantha Asuncion1, Fernando Albelo1, Amanda Tuchler1, Lauren Becker4, Allison Lankford5, Emad Elsamadicy5, Quincy K Tran1,2,3 -
Acute and Critical Care 2024;39(1):138-145.
DOI: https://doi.org/10.4266/acc.2023.01375
Published online: February 15, 2024
1Research Associate Program in Emergency Medicine and Critical Care, Department of Emergency Medicine, University of Maryland School of Medicine, Baltimore, MD, USA
2Department of Emergency Medicine, University of Maryland School of Medicine, Baltimore, MD, USA
3Program in Trauma, University of Maryland School of Medicine, Baltimore, MD, USA
4Division of Pulmonary and Critical Care, Department of Internal Medicine, University of Maryland School of Medicine, Baltimore, MD, USA
5Department of Obstetrics, Gynecology and Reproductive Sciences, University of Maryland School of Medicine, Baltimore, MD, USA
- Corresponding author: Quincy K Tran Department of Emergency Medicine, University of Maryland School of Medicine, 22 South Greene St, P1G01, Baltimore, MD 21201, USA Tel: +1-410-328-4924, Fax: +1-410-328-2876, E-mail: qtran@som.umaryland.edu
- *These authors contributed equally to this work as co-first authors.
© 2024 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 613 Views
- 33 Download
Abstract
-
Background
- Medical complications in peripartum patients are uncommon are uncommon. Often, these patients are transferred to tertiary care centers, but their conditions and outcomes are not well understood. Our study examined peripartum patients transferred to an intensive care unit (ICU) at an academic quaternary center.
-
Methods
- We reviewed charts of adult, non-trauma, interhospital transfer (IHT) peripartum patients sent to an academic quaternary ICU between January 2017 and December 2021. We conducted a descriptive analysis and used multivariable ordinal regression to examine associations of demographic and clinical factors with ICU length of stay (LOS) and hospital length of stay (HLOS).
-
Results
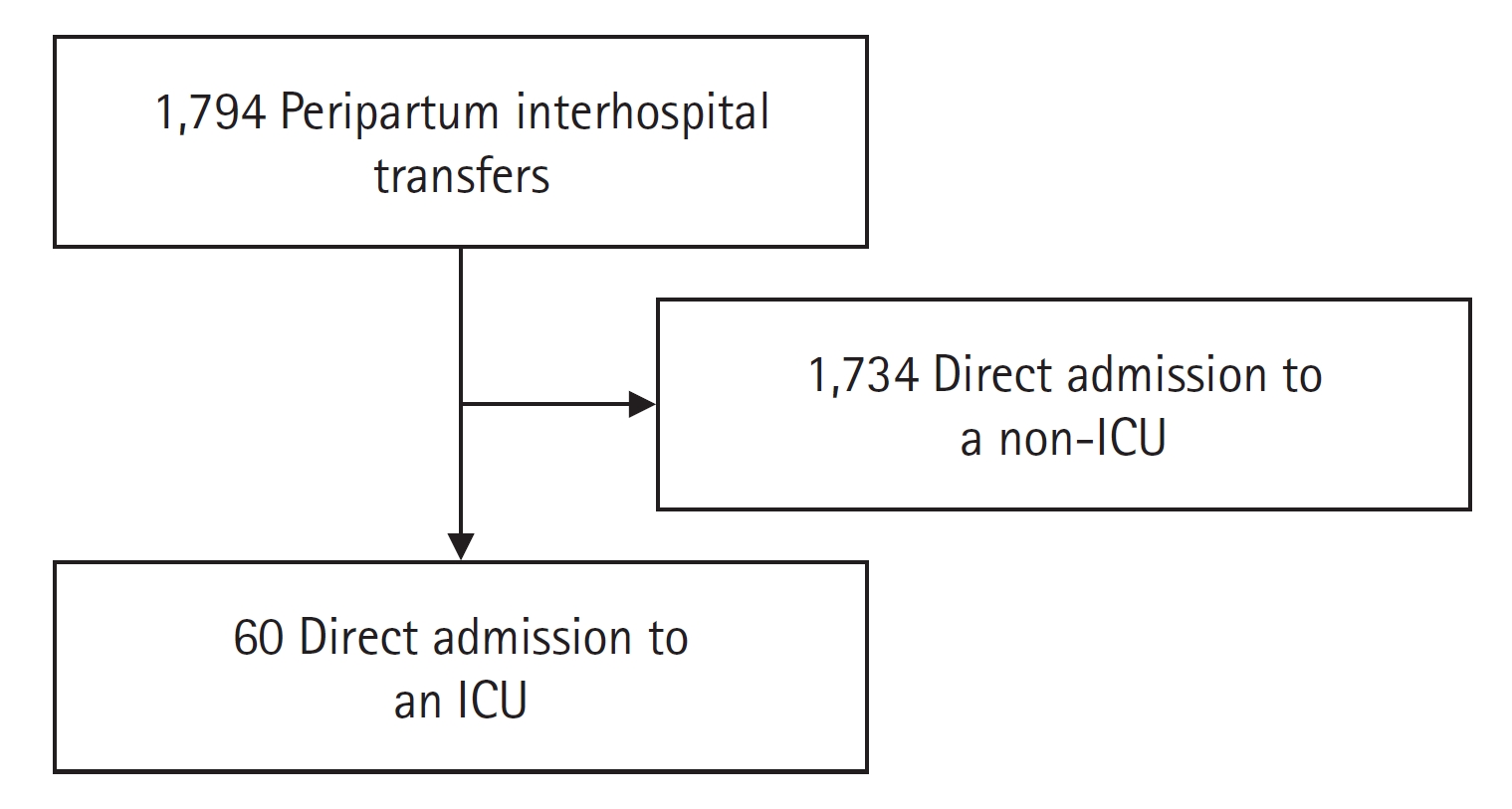
- Of 1,794 IHT peripartum patients, 60 (3.2%) were directly transferred to an ICU. The average age was 32 years, with a median Sequential Organ Failure Assessment (SOFA) score of 3 (1–4.25) and Acute Physiology and Chronic Health Evaluation (APACHE) II score of 8 (7–12). Respiratory failure was most common (32%), followed by postpartum hemorrhage (15%) and sepsis (14%). Intubation was required for 24 (41%), and 4 (7%) needed extracorporeal membrane oxygenation. Only 1 (1.7%) died, while 45 (76.3%) were discharged. Median ICU LOS and HLOS were 5 days (2–12) and 8 days (5–17). High SOFA score was linked to longer HLOS, as was APACHE II.
-
Conclusions
- Transfers of critically ill peripartum patients between hospitals were rare but involved severe medical conditions. Despite this, their outcomes were generally positive. Larger studies are needed to confirm our findings.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
DISCUSSION
KEY MESSAGES
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
FUNDING
None.
-
AUTHOR CONTRIBUTIONS
Conceptualization: KB, AL, EE, QT. Data curation: SP, SA, FA. Formal analysis: JY. Methodology: KB, AT, AL, EE, QT. Project administration: AL, QT. Writing–original draft: SP, KB, QT. Writing–review & editing: LB, QT.
NOTES
Acknowledgments
SUPPLEMENTARY MATERIALS
Supplementary Table 1.
| Variable | Value |
|---|---|
| Age (yr) | 32±6 |
| BMI (kg/m2) | 31.4±8.3 |
| Gravidity | 3.0 (2.0–4.0) |
| Postpartum | 29.0 (48.3) |
| Parity | 2.0 (1.0–3.0) |
| Gestational age (yr) | 30±8 |
| Placenta previa or PAS | 3.0 (5.0) |
| Race | |
| Black | 18.0 (30.0) |
| White | 24.0 (40.0) |
| Hispanic | 7.0 (11.7) |
| Asian | 6.0 (10.0) |
| Other | 5.0 (8.3) |
| Marital status | |
| Single | 25.0 (41.7) |
| Married | 35.0 (58.3) |
| Past medical history | |
| Hypertension | 10.0 (16.7) |
| Asthma | 9.0 (13.3) |
| Diabetes mellitus | 5.0 (8.3) |
| Chronic kidney disease | 2 (3.3) |
| Admission ICU type | |
| Critical care resuscitation unit | 47.0 (78.3) |
| Medical | 8.0 (13.3) |
| Surgical | 3.0 (5.0) |
| Neurocritical care | 2.0 (3.3) |
| Admission diagnosisa) | |
| COVID-19–related respiratory complications | 16.0 (26.7) |
| Postpartum hemorrhage | 9.0 (15.0) |
| Pregnancy-induced hypertensive disorders | 8.0 (13.3) |
| Disease severity score | |
| SOFA score at ICU admission | 3.0 (1.0–4.3) |
| APACHE II score at ICU admission | 10.0 (7.0–12.0) |
| SOFA score 24 hours after admission | 2.0 (0.8–4.0) |
| APACHE II score 24 hours after admission | 5.5 (3.0–9.0) |
| SOFA score at discharge | 1.0 (0.0–3.0) |
| APACHE II score at discharge | 5.0 (2.8–9.3) |
| Discharge disposition | |
| Home | 54.0 (90.0) |
| Acute care (medical/surgical) hospital | 2.0 (3.3) |
| Left against medical advice | 1.0 (1.7) |
| Rehabilitation facility | 1.0 (1.7) |
| Skilled nursing facility | 1.0 (1.7) |
| Deceased | 1.0 (1.7) |
| Length of stay | |
| Total length of stay (day) | 8.8 (4.4–15.6) |
| ICU length of stay (day) | 4.4 (2.1–11.2) |
Values are presented as mean±standard deviation, median (interquartile range), or number (%).
ICU: intensive care unit; BMI: body mass index; PAS: placenta accreta spectrum; COVID-19: coronavirus disease 2019; SOFA: Sequential Organ Failure Assessment; APACHE: Acute Physiology and Chronic Health Evaluation.
a) Only top three diagnoses listed here, see Supplementary Table 1 for full list. One patient may have more than one diagnosis.
| Intervention | No. of patients (%) |
|---|---|
| Intubation | 24 (40.0) |
| Blood transfusion | 20 (33.3) |
| Vasopressor | 13 (21.7) |
| Antihypertensive infusion | 10 (16.7) |
| ECMO cannulation | 2 (3.3) |
| Surgical interventiona) | 24 (40.0) |
| Exploratory laparotomy | 8 (13.3) |
| Dilation and curettage | 3 (5.0) |
| Cesarean | 3 (5.0) |
| Hysterectomy | 2 (3.3) |
| Irrigation and debridement upper extremity | 1 (1.7) |
| Hematoma evacuation | 1 (1.7) |
| Dilation and evacuation | 1 (1.7) |
| Visceral angiogram and gel foam embolization | 1 (1.7) |
| Embolectomy and endovascular stent insertion | 1 (1.7) |
| Cannula removal for prolonged ECMO | 1 (1.7) |
| Central line | 1 (1.7) |
| Tracheostomy | 1 (1.7) |
| Endoscopic ventriculostomy | 1 (1.7) |
| Variableb) | r-value | OR | 95% CI | P-value |
|---|---|---|---|---|
| Age | 0.02 | 1.02 | 0.91–1.13 | 0.76 |
| BMI | 0.01 | 1.01 | 0.93–1.10 | 0.77 |
| Black race | 1.61 | 4.98 | 1.22–20.31 | 0.03 |
| Married | 0.20 | 1.22 | 0.32–4.65 | 0.77 |
| Hypertension | 1.57 | 4.79 | 0.66–34.67 | 0.12 |
| Chronic kidney disease | –0.26 | 0.77 | 0.02–29.51 | 0.89 |
| Asthma | –0.23 | 0.80 | 0.12–5.16 | 0.81 |
| Postpartum | 1.50 | 4.48 | 1.11–18.10 | 0.04 |
| COVID-19 | –1.92 | 0.15 | 0.03–0.78 | 0.02 |
| SOFA score at ICU admission | –0.40 | 0.67 | 0.50–0.91 | 0.01 |
| APACHE II score at ICU admission | –0.16 | 0.85 | 0.72–1.00 | 0.05 |
| Reduction in SOFA score after 24 hours | 0.20 | 1.22 | 0.31–4.84 | 0.78 |
| Reduction in APACHE II score after 24 hours | 0.80 | 2.22 | 0.47–10.42 | 0.31 |
Sommer’s D=0.74, Goodman-Kruskal Gamma=0.74, Kendall’s Tau-a=0.56, Log-likelihood=–56.138.
OR: odds ratio; CI: confidence interval; BMI: body mass index; COVID-19: coronavirus disease 2019; SOFA: Sequential Organ Failure Assessment; ICU: intensive care unit; APACHE: Acute Physiology and Chronic Health Evaluation.
a) Ranked from 0 (0–5 days), 1 (5.1–10 days), 2 (10.1–15 days), and 3 (>15 days); Group 0: n=17 (28.3%), group 1: n=15 (25.0%), group 2: n=12 (20.0%), group 3: n=16 (26.7%);
b) Removed diabetes mellitus due to large confidence interval.
| Variableb) | r-value | OR | 95% CI | P-value |
|---|---|---|---|---|
| Age | –0.02 | 0.98 | 0.89–1.08 | 0.64 |
| BMI | –0.06 | 0.94 | 0.87–1.01 | 0.09 |
| Black race | 0.27 | 1.31 | 0.36–4.76 | 0.68 |
| Married | 0.23 | 1.26 | 0.36–4.35 | 0.72 |
| Hypertension | 0.43 | 1.54 | 0.32–7.34 | 0.59 |
| Asthma | 0.98 | 2.66 | 0.48–14.64 | 0.26 |
| Postpartum | –0.38 | 0.68 | 0.20–2.32 | 0.54 |
| COVID-19 | –1.85 | 0.16 | 0.03–0.77 | 0.02 |
| SOFA score at ICU admission | –0.26 | 0.77 | 0.59–1.02 | 0.07 |
| APACHE II score at ICU admission | –0.16 | 0.85 | 0.74–0.99 | 0.04 |
| Reduction in SOFA score after 24 hours | –0.52 | 0.60 | 0.16–2.19 | 0.44 |
| Reduction in APACHE II score after 24 hours | 1.18 | 3.25 | 0.79–13.32 | 0.10 |
Sommer’s D=0.63, Goodman-Kruskal gamma=0.63, Kendall’s Tau-a=0.48, Log-likelihood=–64.233.
ICU: intensive care unit; OR: odds ratio; CI: confidence interval; BMI: body mass index; COVID-19: coronavirus disease 2019; SOFA: Sequential Organ Failure Assessment; APACHE: Acute Physiology and Chronic Health Evaluation.
a) Ranked from 0 (0–2 days), 1 (2.1–4 days), 2 (4.1–12 days), and 3 (>12 days); Group 0: n=15 (25.0%), group 1: n=13 (21.7%), group 2: n=17 (28.3%), group 3: n=15 (25.0%);
b) Removed diabetes mellitus and chronic kidney disease from model due to large confidence interval.
- 1. Tran QK, Hollis G, Beher R, Abdel-Wahab M, Mester G, Tanveer S, et al. Transport of peripartum patients for medical management: predictors of any intervention during transport. Cureus 2022;14:e31102.ArticlePubMedPMC
- 2. NEMSIS Technical Assistance Center. National EMS database: NEMSIS research data set [Internet]. NEMSIS Technical Assistance Center. 2017;[cited 2023 Dec 20]. Available from: https://nemsis.org/wp-content/uploads/2018/02/NEMSIS-RDS-221-2016-User-Manual.pdf.
- 3. Nawrocki PS, Levy M, Tang N, Trautman S, Margolis A. Interfacility transport of the pregnant patient: a 5-year retrospective review of a single critical care transport program. Prehosp Emerg Care 2019;23:377-84.ArticlePubMed
- 4. O’Brien DJ, Hooker EA, Hignite J, Maughan E. Long-distance fixed-wing transport of obstetrical patients. South Med J 2004;97:816-8.ArticlePubMed
- 5. Jony L, Baskett TF. Emergency air transport of obstetric patients. J Obstet Gynaecol Can 2007;29:406-8.ArticlePubMed
- 6. Akl N, Coghlan EA, Nathan EA, Langford SA, Newnham JP. Aeromedical transfer of women at risk of preterm delivery in remote and rural Western Australia: why are there no births in flight? Aust N Z J Obstet Gynaecol 2012;52:327-33.PubMed
- 7. Elsamadicy E, Plotnikova A, Yang J, Gambhir V, Zahid M, Pirzada S, et al. The utility of severity scoring systems to identify obstetric transports at risk for ICU escalation. Am J Obstet Gynecol 2023;228:S297-8.Article
- 8. Powell E, Sahadzic I, Najafali D, Berman E, Andersen K, Afridi LZ, et al. Is the critical care resuscitation unit sustainable: a 5-year experience of a beneficial and novel model. Crit Care Res Pract 2022;2022:6171598. ArticlePubMedPMCPDF
- 9. Heslehurst N, Ells LJ, Simpson H, Batterham A, Wilkinson J, Summerbell CD. Trends in maternal obesity incidence rates, demographic predictors, and health inequalities in 36,821 women over a 15-year period. BJOG 2007;114:187-94.ArticlePubMed
- 10. Farr A, Lenz-Gebhart A, Einig S, Ortner C, Holzer I, Elhenicky M, et al. Outcomes and trends of peripartum maternal admission to the intensive care unit. Wien Klin Wochenschr 2017;129:605-11.ArticlePubMedPMCPDF
- 11. Lapinsky SE, Hallett D, Collop N, Drover J, Lavercombe P, Leeman M, et al. Evaluation of standard and modified severity of illness scores in the obstetric patient. J Crit Care 2011;26:535. Article
- 12. Porreco RP, Barkey R. Peripartum intensive care. J Matern Fetal Neonatal Med 2010;23:1136-8.ArticlePubMed
- 13. Cojocaru L, Turan OM, Levine A, Sollecito L, Williams S, Elsamadicy E, et al. Proning modus operandi in pregnancies complicated by acute respiratory distress syndrome secondary to COVID-19. J Matern Fetal Neonatal Med 2022;35:9043-52.ArticlePubMed
- 14. Beigmohammadi MT, Amoozadeh L, Rezaei Motlagh F, Rahimi M, Maghsoudloo M, Jafarnejad B, et al. Mortality predictive value of APACHE II and SOFA scores in COVID-19 patients in the intensive care unit. Can Respir J 2022;2022:5129314. ArticlePubMedPMCPDF
- 15. Suri J, Khanam Z. Prognosticating fetomaternal ICU outcomes. Indian J Crit Care Med 2021;25(Suppl 3):S206-22.ArticlePubMedPMC
- 16. Khergade M, Suri J, Bharti R, Pandey D, Bachani S, Mittal P. Obstetric early warning score for prognostication of critically ill obstetric patient. Indian J Crit Care Med 2020;24:398-403.ArticlePubMedPMC
- 17. Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA 2016;315:788-800.ArticlePubMed
- 18. Aldawood A. Clinical characteristics and outcomes of critically ill obstetric patients: a ten-year review. Ann Saudi Med 2011;31:518-22.ArticlePubMedPMC
- 19. Miller T, Emamian N, Glick Z, Chen N, Cao T, Buganu A, et al. Association between resuscitation in the critical care resuscitation unit and in-hospital mortality. Am J Emerg Med 2022;60:96-100.ArticlePubMed
References
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-

- We recommend
- Related articles
-
- Characteristics and outcomes of patients with chronic obstructive pulmonary disease admitted to the intensive care unit due to acute hypercapnic respiratory failure
- Characteristics and prognostic factors of very elderly patients admitted to the intensive care unit
- Clinical characteristics and outcomes of critically ill COVID-19 patients in Sfax, Tunisia

