Development of a prognostic scoring system in patients with pneumonia requiring ventilator care for more than 4 days: a single-center observational study
Article information

Abstract
Background
The aim of the present study was to develop a prognostic model using demographic characteristics, comorbidities, and clinical variables measured on day 4 of mechanical ventilation (MV) for patients with prolonged acute mechanical ventilation (PAMV; MV for >96 hours).
Methods
Data from 437 patients (70.9% male; median age, 68 years) were obtained over a period of 9 years. All patients were diagnosed with pneumonia. Binary logistic regression identified factors predicting mortality at 90 days after the start of MV. A PAMV prognosis score was calculating ß-coefficient values and assigning points to variables.
Results
The overall 90-day mortality rate was 47.1%. Five factors (age ≥65 years, body mass index <18.5 kg/m2, hemato-oncologic diseases as comorbidities, requirement for vasopressors on day 4 of MV and requirement for neuromuscular blocking agents on day 4 of MV) were identified as prognostic indicators. Each factor was valued as +1 point, and used to develop a PAMV prognosis score. This score showed acceptable discrimination (area under the receiver operating characteristic curve of 0.695 for mortality, 95% confidence interval 0.650–0.738, p<0.001), and calibration (Hosmer–Lemeshow chi-square=6.331, with df 7 and p=0.502). The cutoff value for predicting mortality based on the maximum Youden index was ≤2 (sensitivity, 87.5%; specificity, 41.3%). For patients with PAMV scores ≤1, 2, 3 and ≥4, the 90-day mortality rates were 29.2%, 45.7%, 67.9%, and 90.9%, respectively (P<0.001).
Conclusions
Our study developed a PAMV prognosis score for predicting 90-day mortality. Further research is needed to validate the utility of this score.
INTRODUCTION
Advances in the early management of acute critically ill patients requiring ventilator care have led to long-term stays in the intensive care unit (ICU), which pose a high clinical and financial burden. Notably, critical care resources and facilities at university-affiliated tertiary care hospitals in Korea are typically more limited than those in North America and Europe [1,2]. Furthermore, patients’ families or surrogates usually want to know a patient’s medical status and likely clinical outcome if the patient is placed on mechanical ventilation (MV). Therefore, developing strategies to improve outcomes and establishing long-term care plans for patients at the early stage of MV is necessary.
Recent studies have described a novel subpopulation of patients on ventilator care that require MV for more than 96 hours, and these patients are referred to as “prolonged acute mechanical ventilation (PAMV)” cases [3,4]. This subpopulation is categorized as patients with “chronic critical illness” (CCI) [5] and is projected to increase over the next years [3]. If a PAMV case still shows severe illness on day 4 of MV, the long-term prognosis is likely to be poor. However, few studies have examined factors that affect the long-term prognosis of these patients.
Based on a report about factors that are prognostic for 28-day mortality [6], we hypothesized that some clinical variables on day 4 of MV may be useful for predicting the long-term prognosis of PAMV patients. Previous studies have suggested that demographic characteristics, body mass index (BMI), and comorbidities have prognostic value in patients with critical illness [7-10]. If these clinical parameters can be used to predict prognosis, it would be of great help to critical care physicians with respect to treatment planning at the early stage of ventilator care.
In the present study, we evaluated prognostic indicators that are useful for predicting the 90-day mortality of patients on PAMV. We also constructed a mortality prediction model (PAMV prognosis score) based on the prognostic factors. In addition, we compared the ability of this new PAMV prognosis score with that of two commonly used severity of illness scores (Acute Physiology and Chronic Health Evaluation [APACHE] II and Sequential Organ Failure Assessment [SOFA]) to predict mortality.
MATERIALS AND METHODS
In our study, the relevant medical, laboratory, and radiological data were extracted and used to fill out a case report form for each patient. These data were then analyzed. The study protocol was approved by the Institutional Review Board of Pusan National University Hospital (IRB No. 2003-012-088). Due to the retrospective and observational nature of our study, the need for informed consent from enrolled subjects or their surrogates was waived. The study had no impact on the treatment of enrolled patients.
Study Design and Patient Selection
This retrospective, observational study was conducted in the medical ICU of a 1,200 bed university-affiliated tertiary care hospital. This medical ICU has full cardiovascular facilities and close airway monitoring equipment, with a nurse-to-bed ratio of 1:3. All subjects were managed according to therapeutic recommendations (based on a lung-protective ventilator strategy) [11].
Data from patients treated between March 1, 2008 and February 28, 2017 were evaluated retrospectively. All adult subjects (≥ 18 years old) who were admitted to the medical ICU were assessed for eligibility; patients who were admitted to the coronary care unit were excluded. Patients diagnosed with pneumonia (community- and hospital-acquired pneumonia ([CAP] and [HAP]) and receiving ventilator care for more than 96 hours (defined as PAMV) [4,12] were included. Patients whose primary reason for ventilator care was not pneumonia were excluded, as were patients who received tracheostomy prior to hospital admission or less than 3 days after ICU admission; this is because early tracheostomy introduces bias when predicting prognosis (Figure 1). The definition of CAP and HAP was applied to enrolled patients; the definitions were based on those in the literature [13,14].
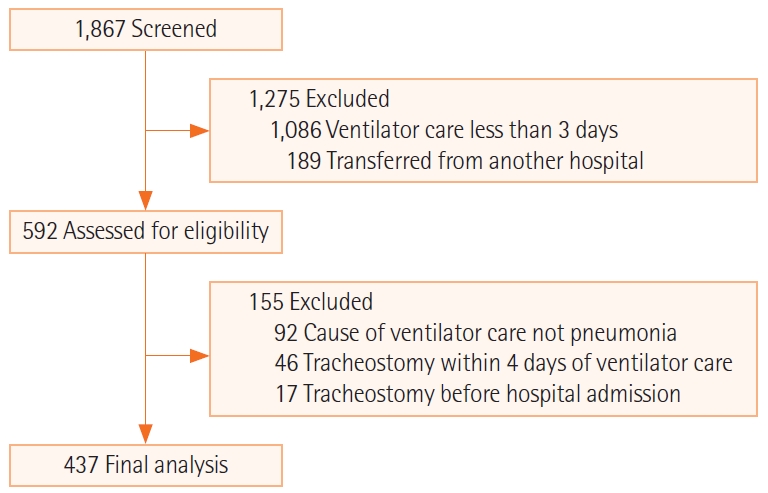
Flowchart of recruited and enrolled study participants.
Data Collection
Demographic and clinical data were obtained retrospectively from electronic medical records; these data included age, sex, BMI, length of stay (LOS) in the ICU and hospital, and duration of MV. Severity of illness was measured using the APACHE II score; accompanying organ failure was assessed using the SOFA score [15,16]. The APACHE II and SOFA scores were calculated from laboratory and clinical data obtained within the first 24 hours of ICU admission. On admission, the underlying comorbidities of all enrolled subjected were gathered from medical records. In addition, Charlson’s weighted index of comorbidities (WIC) was evaluated, as previous studies demonstrated the prognostic utility of this index in PAMV patients [17,18].
Studies have reported that some clinical variables are prognostic factors in patients under ventilator care [6,19-22]. Therefore, the following laboratory and clinical data obtained on day 4 of MV were recorded: complete blood count, the lowest PaO2/FiO2 ratio, the need of vasopressors and hemodialysis, and unavoidable requirement of neuromuscular blocking agents (NMBAs) due to ventilator dyssynchrony (intermittent or continuous). We also recorded the following clinical variables on day 4 of MV, based on studies about severity and prognosis of CAP [23,24]: serum albumin, blood urea nitrogen (BUN), pH on arterial blood gas analysis, and simple chest radiograph. Lactic acid level was obtained on same day because accompanying septic shock would be important in predicting prognosis [25].
The ICU, in-hospital, and 90-day cumulative mortality rates after ventilator care were assessed. With respect to surviving patients discharged from hospital, the 90-day mortality rate was obtained from the National Health Insurance Service Database. The primary outcome measure was 90-day mortality.
Statistical Analysis
Continuous variables are expressed as the median (range) and were compared using the Student t-test or Mann-Whitney U-test, as applicable. Categorical variables are expressed as numbers (percentages) and were compared using the chi-square test or Fisher’s exact test (for small numbers), as applicable. Stepwise logistic regression analysis was used to identify factors that are independent predictors of 90-day mortality. In addition, β-coefficients derived from multiple logistic regression were simplified and presented as natural numbers > 0; these were calculated as the sum of the simplified β-coefficients, as previously described [19-22,26]. The prognostic model (PAMV prognosis score) was developed based on the sum of the β-coefficients. To predict 90-day survival, Kaplan-Meier estimates were stratified according to the score, and curves were compared using the log-rank test. The areas under the receiver operating characteristic curve (AUCs) were used to assess the discriminatory ability of the prognostic model. In addition, model calibration was assessed using the Hosmer–Lemeshow test. The AUCs of all prognostic models were compared with those of the APACHE II and SOFA scores using the DeLong test, as described previously [27]. An optimal cutoff value was identified based on the maximum Youden’s index [28]. The sensitivity (SS), specificity (SP), positive likelihood ratio (PLR), negative likelihood ratio (NLR), positive predictive value (PPV), and negative predictive value (NPV) for predicting mortality were determined. All tests were two-tailed and P-values < 0.05 were considered statistically significant. All statistical analyses were performed using IBM SPSS ver. 24.0 (IBM Corp., Armonk, NY, USA) and MedCalc ver. 19.4 (MedCalc Software, Ostend, Belgium).
RESULTS
Patient Characteristics
During the study period, a total of 1,867 patients received ventilator care. After application of exclusion criteria, 437 were eligible for inclusion in the study (Figure 1). The ICU, in-hospital, and 90-day cumulative mortality rates were 35.2% (n=154), 39.1% (n=171), and 47.1% (n=206), respectively. Table 1 shows the baseline characteristics of the patient group and compares survivors and non-survivors at 90 days after ventilator care. Non-survivors were older, had a lower BMI, and shorter ICU, hospital, and ventilator LOS than survivors. Non-survivors also had higher APACHE II and SOFA scores on ICU admission and Charlson’s WIC than survivors. With respect to comorbidities, non-survivors had a significantly higher rate of chronic lung diseases (chronic obstructive pulmonary disease, interstitial lung disease, bronchiectasis, and tuberculosis-destroyed lung) and hemato-oncologic disease than survivors (Table 1). Comparison of clinical variables on day 4 of ventilator care revealed that non-survivors were more likely to require vasopressors and NMBAs than survivors. In addition, the percentages of patients with PaO2/FiO2 <200 mm Hg, platelet count < 100 × 109/L, BUN > 7 mmol/L, pH < 7.35, and lactic acid > 2.0 mmol/L were significantly higher in non-survivors than among survivors (Table 1).

Clinical characteristics of survivors and non-survivors
Prognostic Factors Associated with 90-Day Mortality
Univariate and multivariate analyses of risk factors predicting 90-day mortality are shown in Table 2. Multivariate analyses identified age ≥ 65 years, BMI < 18.5 kg/m2, hemato-oncologic diseases as comorbidities, and two clinical parameters on day 4 of ventilator care (requirement of vasopressors and NMBAs) as significant prognostic indicators of 90-day mortality.

Logistic regression analysis of mortality in all patients
A Prognostic Model for Predicting 90-Day Mortality
Based on the β-coefficients observed in multivariate analyses, a PAMV prognosis score was developed based on all of the factors; each factor was valued as +1 point. This score showed acceptable discrimination (AUC of 0.695 for mortality; 95% confidence interval [CI], 0.650–0.738; P<0.001) and calibration (Hosmer -Lemeshow chi-square = 6.331, with df 7 and P=0.502) (Figure 2). The cutoff value for predicting mortality based on the maximum Youden index was ≤ 2 (SS, 87.5%; SP, 41.3%; PLR, 2.2; NLR, 0.7; PPV, 62.5%; and NPV, 74.6%). Kaplan-Meier survival curves based on the model score were obtained for 90-day mortality relative to the score for this model (Figure 2). As the score increased, so did the mortality rate (score ≤ 1, 2, 3, and ≥ 4 = 90-day mortality rates of 29.2%, 45.7%, 67.9%, and 90.9%, respectively) (P<0.001).
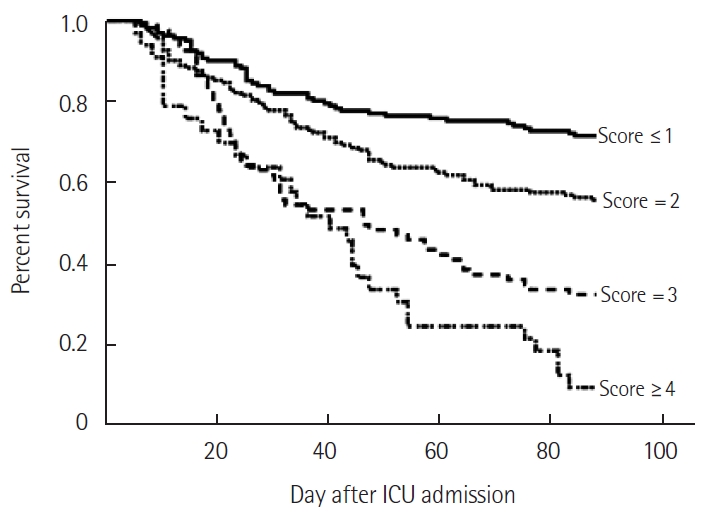
Kaplan–Meier survival curves, stratified according to the prolonged acute mechanical ventilation prognosis score (log-rank <0.001). ICU: intensive care unit.
For all patients, the AUCs for the PAMV prognosis, SOFA, and APACHE II scores were 0.695 (95% CI, 0.650–0.738; P<0.001), 0.608 (95% CI, 0.561–0.654; P<0.001), and 0.569 (95% CI, 0.521–0.616; P<0.001), respectively. Comparison of the AUCs of this model with those of these two severity of illness scores revealed that the AUC of the PAMV prognosis score were significantly higher than those of the two scores (P=0.009 and P=0.001, respectively (Figure 3).
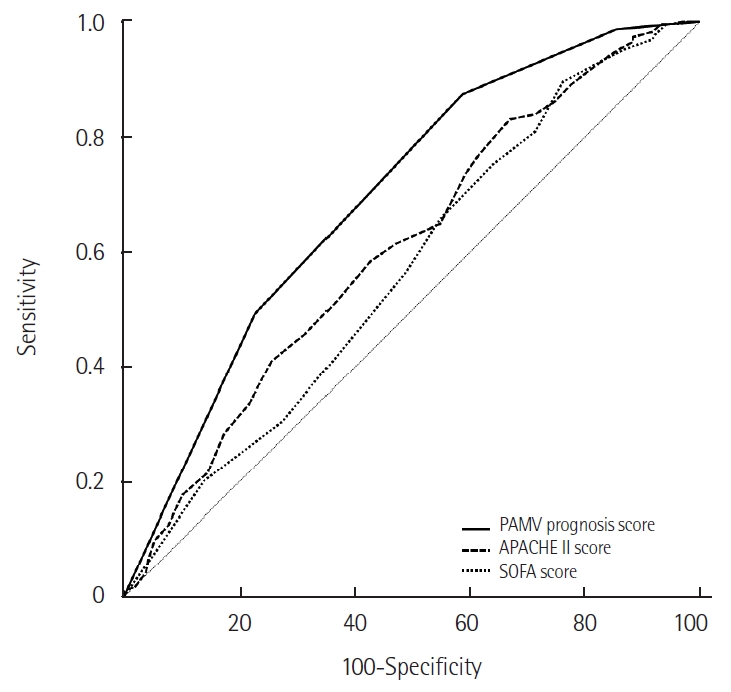
Comparison of receiver operating characteristic (ROC) curves for the prolonged acute mechanical ventilation (PAMV) prognosis score, Acute Physiology and Chronic Health Evaluation (APACHE) II score, and Sequential Organ Failure Assessment (SOFA) score for predicting 90-day mortality. For all patients, the areas under the ROC curve (AUCs) for the PAMV prognosis score, SOFA score, and APACHE II score were 0.695 (95% CI, 0.650–0.738; P<0.001), 0.608 (95% CI, 0.561–0.654; P<0.001), and 0.569 (95% CI, 0.521–0.616; P<0.001), respectively. The AUC for the PAMV prognosis score was significantly higher than that of the other two scores (P=0.009 and P=0.001, respectively). CI: confidence interval.
DISCUSSION
The present study evaluated prognostic factors in PAMV patients diagnosed with pneumonia in a medical ICU. The analysis identified older age, being underweight, hemato-oncologic diseases as comorbidities, and clinical factors (requirement of vasopressors and NMBAs) on day 4 of MV as useful predictors of 90-day mortality. These indicators are readily applicable to these patients because they have been noted as prognostic factors in various reports in the field of critical care medicine [6,7,9,20-22,29].
The results were used to develop a prediction model. The model showed good discrimination and calibration for predicting mortality. Based on the AUCs, the model was not inferior to the APACHE and SOFA scores obtained on the day of admission. Our PAMV prognosis model is objective and easy to extract, making it easy to link to electronic medical records to inform clinical care. Although this model should not override clinical judgment, the present study suggests that the model would help critical care physicians inform the patients’ family or surrogates about the likely LOS in the ICU when a patient is placed on MV. However, the model requires further validation in large-scale multicenter studies.
The prevalence, long-term mortality, and costs of CCI are substantial [5]; therefore, prognostic models for predicting long-term outcomes have been developed using the clinical variables of patients on ventilator care. The ProVent score was validated to predict 1-year mortality in patients requiring prolonged MV (defined as more than 21 days of MV) [21,30,31]. This score is based on four variables readily assessed on day 21 of MV: a requirement for dialysis, a requirement for vasopressors, age ≥ 50 or ≥ 65 years, and a platelet count < 150 × 109/L. In addition, the extended ProVent model included comorbidities and laboratory data (albumin, bilirubin) [9]. Currently, the ProVent14 score is used to predict 1-year mortality in patients requiring MV for more than 14 days; this score is derived by assessing clinical variables on day 14 of MV. These variables include a requirement for dialysis, a requirement for vasopressors, age ≥ 50 or ≥ 65 years, a platelet count < 100 × 109/L, and a non-trauma diagnosis [19,22]. A study of PAMV patients identified four variables on day 4 of MV (a requirement for vasopressors, a requirement for NMBAs, a requirement for dialysis, and a BMI ≤ 21 kg/m2) as independent factors predictive of 28-day mortality [6]. The major advantage of the above-mentioned models is their simplicity, which means that they can be used in clinical practice and help inform management decisions regarding patients on MV. Herein, we included five clinical factors in developing the prognostic model, which is useful for predicting mortality. However, our PAMV prognosis model is not ideal for assessing prognosis in critically ill patients on MV, which raise several considerations. First, other clinical variables (such as PaO2/FiO2 < 200 mm Hg, platelet count < 100 × 109/L, albumin < 3.5 g/dL, BUN > 7 mmol/L, pH < 7.35, lactic acid > 2.0 mmol/L, and serum sodium ≥ 145 mmol/L) are reported as prognostic factors in critically ill patients [19,23-25,32]. Other research may find that these parameters are prognostic factors of PAMV patients. Second, clinical outcomes are affected by multiple extraneous factors, including the perspectives of the patient’s family or surrogates, physician-family communications, and the utilization of medical resources. Third, critical care resources and facilities at university hospitals are limited, which also affects prognosis [1,33]. Therefore, developing new prediction models for patients requiring early stage ventilator care and for those requiring long-term ventilator care is necessary. In addition to clinical variables, socioeconomic, and ethical issues should be included in prognostic models and examined in large-scale multicenter studies.
The present study had several limitations. First, the study was conducted in the medical ICU of a single-center institution; therefore, the data may not be generalizable to other settings. Second, we hypothesized that the prognostic model would differ according to CAP and VAP; however, we could not accurately distinguish between these diagnoses due to the retrospective nature of the study. Third, other clinical variables such as organ dysfunction on day 4 of MV, or other comorbidities, could be considered for inclusion in the prognostic model; however, we found no such additional prognostic factors, which may be because of incomplete medical records. Finally, our study investigated prognostic factors for PAMV patients with a diagnosis of pneumonia; patients requiring PAMV due to other causes would need a different prognostic model. Further studies based on heterogeneous populations are needed to develop such prognostic models.
In conclusion, to the best of our knowledge, this study is the first to develop a prognostic model for predicting 90-day mortality in PAMV patients based on clinical variables on day 4 of MV, comorbidities, and BMI. Large-scale multicenter studies are needed to evaluate additional useful prognostic indicators and to develop new prognostic models with a higher power to predict long-term mortality. Such models will aid decision-making by critical care physicians at the early stage of MV.
KEY MESSAGES
▪ Developing strategies for the early stage of ventilator care are necessary to improve outcomes and establish a long-term care plan.
▪ A prognostic model based on older age, low body mass index, hemato-oncologic diseases as comorbidities, and clinical variables on day 4 of MV (requirement for vasopressors and neuromuscular blocking agents) is useful for predicting 90-day mortality in patients with pneumonia requiring ventilator care for more than 4 days.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: all authors. Data curation & Formal analysis: YO, YK. Funding acquisition: KL. Methodology, Project administration, Visualization, & Writing–original draft: all authors. Writing–review & editing: KL.
Acknowledgements
This work was supported by a clinical research grant from Pusan National University Hospital (2020).