Articles
- Page Path
- HOME > Acute Crit Care > Volume 36(4); 2021 > Article
-
Original Article
Infection Association of vitamin D deficiency with COVID-19 severity and mortality in Iranian people: a prospective observational study -
Alireza Fatemi1
 , Seyed Hossein Ardehali2, Ghazaleh Eslamian3, Morvarid Noormohammadi4, Shirin Malek5
, Seyed Hossein Ardehali2, Ghazaleh Eslamian3, Morvarid Noormohammadi4, Shirin Malek5 -
Acute and Critical Care 2021;36(4):300-307.
DOI: https://doi.org/10.4266/acc.2021.00605
Published online: November 29, 2021
1Men's Health and Reproductive Health Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2Department of Anesthesiology and Critical Care, Shohadaye Tajrish Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran
3Department of Cellular and Molecular Nutrition, Faculty of Nutrition and Food Technology, National Nutrition and Food Technology Research Institute, Shahid Beheshti University of Medical Sciences, Tehran, Iran
4Student Research Committee, Faculty of Nutrition and Food Technology, National Nutrition and Food Technology Research Institute, Shahid Beheshti University of Medical Sciences, Tehran, Iran
5Department of Nutrition and Food Science, California State University, Chico, CA, USA
- Corresponding author: Ghazaleh Eslamian Department of Cellular and Molecular Nutrition, Faculty of Nutrition and Food Technology, National Nutrition and Food Technology Research Institute, Shahid Beheshti University of Medical Sciences, No 7, Hafezi St, Farahzadi Blvd, P.O. Box 19395-4741, Tehran 1981619573, Iran Tel: +98-21-22360658, Fax: +98-21-22360657, E-mail: gh.eslamian@sbmu.ac.ir
Copyright © 2021 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background
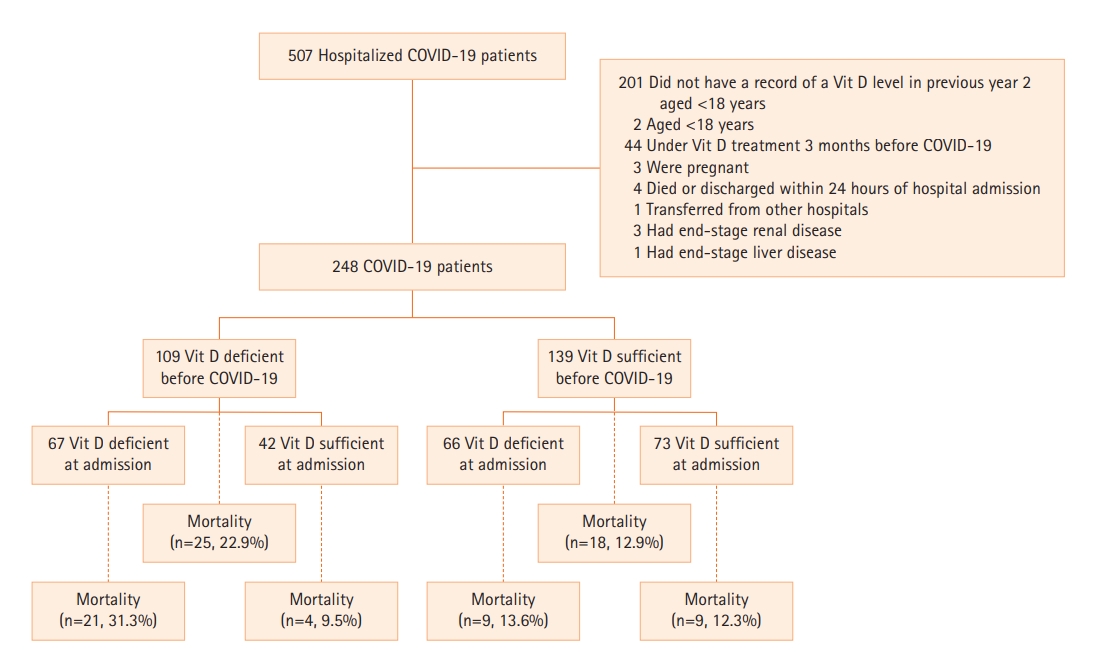
- As the coronavirus disease 2019 (COVID-19) pandemic continues to escalate, it is important to identify the prognostic factors related to increased mortality and disease severity. To assess the possible associations of vitamin D level with disease severity and survival, we studied 248 hospitalized COVID-19 patients in a single center in a prospective observational study from October 2020 to May 2021 in Tehran, Iran.
-
Methods
- Patients who had a record of their 25-hydroxyvitamin D level measured in the previous year before testing positive with COVID-19 were included. Serum 25-hydroxyvitamin D level was measured upon admission in COVID-19 patients. The associations between clinical outcomes of patients and 25-hydroxyvitamin D level were assessed by adjusting for potential confounders and estimating a multivariate logistic regression model.
-
Results
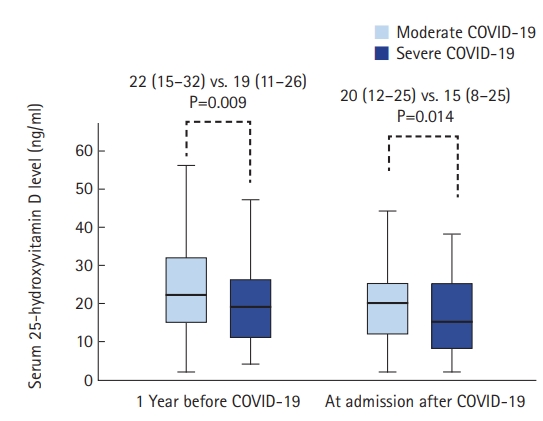
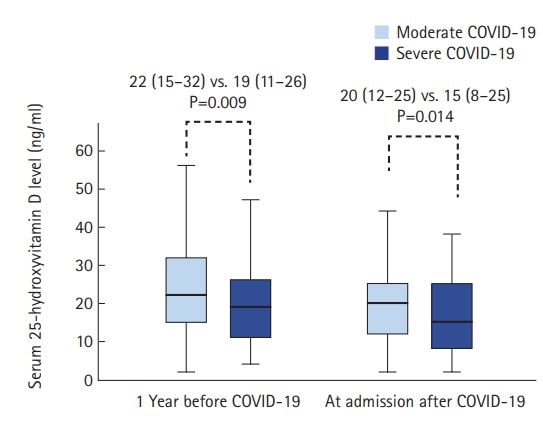
- The median (interquartile range) age of patients was 60 years (44–74 years), and 53% were male. The median serum 25-hydroxyvitamin D level prior to admission decreased with increasing COVID-19 severity (P=0.009). Similar findings were obtained when comparing median serum 25-hydroxyvitamin D on admission between moderate and severe patients (P=0.014). A univariate logistic regression model showed that vitamin D deficiency prior to COVID-19 was associated with a significant increase in the odds of mortality (odds ratio, 2.01; P=0.041). The multivariate Cox model showed that vitamin D deficiency on admission was associated with a significant increase in risk for mortality (hazard ratio, 2.35; P=0.019).
-
Conclusions:
- Based on our results, it is likely that deficient vitamin D status is associated with increased mortality in COVID-19 patients. Thus, evaluating vitamin D level in COVID-19 patients is warranted.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
DISCUSSION
HIGHLIGHTS
-
CONFLICT OF INTEREST No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conceptualization: AF, SHA, GE. Data curation: GE, SM. Formal analysis: SHA, GE, MN. Funding acquisition: AF, SHA, GE, MN. Methodology: AF, SHA, GE, SM. Project administration: GE. Visualization: AF, MN. Writing–original draft: AF, SHA, GE. Writing–review & editing: all authors.
NOTES
| Variable | Overall |
1 Year before COVID-19 positive test |
At admission | ||||
|---|---|---|---|---|---|---|---|
|
Vitamin D classification |
Vitamin D classification |
||||||
| <20 ng/ml | ≥20 ng/ml | P-value | <20 ng/ml | ≥20 ng/ml | P-value | ||
| No. of patients | 248 | 109 | 139 | 133 | 115 | ||
| Age (yr) | 60 (44–74) | 65 (49–75) | 55 (38–70) | 0.002a,b | 61 (47–75) | 58 (36–70) | 0.033a,b |
| Sex | 0.439c | 0.957c | |||||
| Male | 132 (53.2) | 55 (50.5) | 77 (55.4) | 71 (53.4) | 61 (53) | ||
| Female | 116 (46.8) | 54 (49.5) | 62 (44.6) | 62 (46.6) | 54 (47) | ||
| Educational level | 0.461c | 0.757c | |||||
| Primary/secondary school | 38 (15.3) | 20 (18.3) | 18 (12.9) | 20 (15) | 18 (15.7) | ||
| Bachelor's degree | 167 (67.3) | 72 (66.1) | 95 (68.3) | 92 (69.2) | 75 (65.2) | ||
| Master's/doctoral degree | 43 (17.3) | 17 (15.6) | 26 (18.7) | 21 (15.8) | 22 (19.1) | ||
| Severity of COVID-19 | 0.006a,c | 0.018a,c | |||||
| Moderate | 162 (65.3) | 61 (56) | 101 (72.7) | 78 (58.6) | 84 (73) | ||
| Severe | 86 (34.7) | 48 (44) | 38 (27.3) | 55 (41.4) | 31 (27) | ||
| Body mass index (kg/m2) | 27.5 (25–33.5) | 26.1 (25–33.2) | 28 (25–33.8) | 0.156b | 27.2 (25–33.8) | 27.5 (25–32.7) | 0.897b |
| Body mass index ≥30 kg/m2 | 93 (37.5) | 35 (32.1) | 58 (41.7) | 0.121c | 52 (39.1) | 41 (35.7) | 0.576c |
| Comorbidity | |||||||
| Diabetes | 55 (22.2) | 28 (25.7) | 27 (19.4) | 0.239c | 32 (24.1) | 23 (20) | 0.443c |
| Hypertension | 83 (33.5) | 41 (37.6) | 42 (30.2) | 0.220c | 42 (31.6) | 41 (35.7) | 0.498c |
| Pulmonary circulation disorder | 17 (6.9) | 9 (8.3) | 8 (5.8) | 0.439c | 8 (6) | 9 (7.8) | 0.574c |
| Chronic pulmonary disease | 63 (25.4) | 25 (22.9) | 38 (27.3) | 0429c | 36 (27.1) | 27 (23.5) | 0.517c |
| Chronic kidney disease | 50 (20.2) | 25 (22.9) | 25 (18) | 0.335c | 28 (21.1) | 22 (19.1) | 0.707c |
| Liver disease | 22 (8.9) | 10 (9.2) | 12 (8.6) | 0.882c | 9 (6.8) | 13 (11.3) | 0.210c |
| Immunocompromised state | 58 (23.4) | 30 (27.5) | 28 (20.1) | 0.173c | 26 (19.5) | 32 (27.8) | 0.125c |
| Depression | 49 (19.8) | 27 (24.8) | 22 (15.8) | 0.079c | 31 (23.3) | 18 (15.7) | 0.131c |
| Laboratory data | |||||||
| Total leucocyte count | 7,856 (5,856–11,165) | 8,002 (5,929–12,183) | 7,850 (5,854–10,901) | 0.403b | 8,502 (5,856–12,735) | 7,660 (5,803–10,012) | 0.160b |
| Lymphocyte count | 22.8 (17–31.5) | 22.8 (17–31.7) | 22.8 (17–30.8) | 0.877b | 23.3 (16.7–35.6) | 22.3 (17–29.1) | 0.464b |
| CRP level (mg/dl) | 4.50 (3.35–6.08) | 5.01 (3.66–6.31) | 4.40 (3.21–6.01) | 0.052b | 5.02 (4.01–6.31) | 4.03 (2.51–5.90) | 0.001a,b |
| D-dimer (ng/ml) | 854 (522–1,240) | 874 (521–1,499) | 852 (525–987) | 0.027a,b | 874 (755–1,437) | 854 (485–984) | 0.002a,b |
| O2 saturation (%) | 88 (85–89) | 87 (85–89) | 88 (87–89) | 0.066b | 88 (86–89) | 87 (85–90) | 0.144b |
| Clinical outcomes | |||||||
| Mortality | 43 (17.3) | 25 (22.9) | 18 (12.9) | 0.039a,c | 30 (22.6) | 13 (11.3) | 0.020a,c |
| Hospital length of stay (day) | 9 (7–14) | 9 (5–14) | 9 (7–15) | 0.062b | 9 (7–14) | 8 (6–14) | 0.197b |
Values are presented as median (interquartile range) or number (%) unless otherwise indicated.
25(OH)D: 25-hydroxyvitamin D; COVID-19: coronavirus disease 2019; OR: odds ratio; CI: confidence interval; BMI: body mass index; CRP: C-reactive protein.
a Multivariable analyses were conducted using logistic regression models utilizing the simultaneous method.
Values are presented as median (interquartile range) or number (%) unless otherwise indicated.
25(OH)D: 25-hydroxyvitamin D; COVID-19: coronavirus disease 2019; HR: hazard ratio; CI: confidence interval; BMI: body mass index; CRP: C-reactive protein.
a Multivariable analyses were conducted using Cox regression models utilizing the simultaneous method.
- 1. Worldometer. COVID-19 corona virus pandemic. Worldometer; 2021 [cited 2021 May 10]. Available from: https://www.worldometers.info/coronavirus/ .2021.
- 2. Weiss P, Murdoch DR. Clinical course and mortality risk of severe COVID-19. Lancet 2020;395:1014-5.ArticlePubMedPMC
- 3. Holick MF. The vitamin D deficiency pandemic: approaches for diagnosis, treatment and prevention. Rev Endocr Metab Disord 2017;18:153-65.ArticlePubMed
- 4. Charoenngam N, Holick MF. Immunologic effects of vitamin d on human health and disease. Nutrients 2020;12:2097. ArticlePubMedPMC
- 5. Zdrenghea MT, Makrinioti H, Bagacean C, Bush A, Johnston SL, Stanciu LA. Vitamin D modulation of innate immune responses to respiratory viral infections. Rev Med Virol 2017;27:e1909. Article
- 6. Luo X, Liao Q, Shen Y, Li H, Cheng L. Vitamin D deficiency is associated with COVID-19 Incidence and disease severity in Chinese people [corrected]. J Nutr 2021;151:98-103.ArticlePubMed
- 7. Aslan MT, Aslan İÖ, Özdemir Ö. Letter to the editor: is vitamin d one of the key elements in COVID-19 days? J Nutr Health Aging 2020;24:1038-9.ArticlePubMedPMC
- 8. Herr C, Shaykhiev R, Bals R. The role of cathelicidin and defensins in pulmonary inflammatory diseases. Expert Opin Biol Ther 2007;7:1449-61.ArticlePubMed
- 9. Agier J, Efenberger M, Brzezińska-Błaszczyk E. Cathelicidin impact on inflammatory cells. Cent Eur J Immunol 2015;40:225-35.PubMedPMC
- 10. Yisak H, Ewunetei A, Kefale B, Mamuye M, Teshome F, Ambaw B, et al. Effects of vitamin D on COVID-19 infection and prognosis: a systematic review. Risk Manag Healthc Policy 2021;14:31-8.ArticlePubMedPMC
- 11. Liu N, Sun J, Wang X, Zhang T, Zhao M, Li H. Low vitamin D status is associated with coronavirus disease 2019 outcomes: a systematic review and meta-analysis. Int J Infect Dis 2021;104:58-64.ArticlePubMedPMC
- 12. Pereira M, Dantas Damascena A, Galvão Azevedo LM, de Almeida Oliveira T, da Mota J. Vitamin D deficiency aggravates COVID-19: systematic review and meta-analysis. Crit Rev Food Sci Nutr 2020 Nov 4 [EPUB]. https://doi.org/10.1080/10408398.2020.1841090.Article
- 13. World Health Organization. Clinical management of severe acute respiratory infection when novel coronavirus (2019-nCoV) infection is suspected: interim guidance, 28 January 2020 [Internet]. Geneva: World Health Organization; 2020 [cited 2021 May 10]. Available from: https://apps.who.int/iris/handle/10665/330893.
- 14. Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2011;96:1911-30.ArticlePubMed
- 15. Bhatraju PK, Ghassemieh BJ, Nichols M, Kim R, Jerome KR, Nalla AK, et al. COVID-19 in critically ill patients in the Seattle Region: case series. N Engl J Med 2020;382:2012-22.ArticlePubMed
- 16. Ilie PC, Stefanescu S, Smith L. The role of vitamin D in the prevention of coronavirus disease 2019 infection and mortality. Aging Clin Exp Res 2020;32:1195-8.ArticlePubMedPMC
- 17. D'Avolio A, Avataneo V, Manca A, Cusato J, De Nicolò A, Lucchini R, et al. 25-Hydroxyvitamin D concentrations are lower in patients with positive PCR for SARS-CoV-2. Nutrients 2020;12:1359. ArticlePubMedPMC
- 18. Meltzer DO, Best TJ, Zhang H, Vokes T, Arora V, Solway J. Association of vitamin D status and other clinical characteristics with COVID-19 test results. JAMA Netw Open 2020;3:e2019722. ArticlePubMedPMC
- 19. Radujkovic A, Hippchen T, Tiwari-Heckler S, Dreher S, Boxberger M, Merle U. Vitamin D deficiency and outcome of COVID-19 patients. Nutrients 2020;12:2757. ArticlePubMedPMC
- 20. Tehrani S, Khabiri N, Moradi H, Mosavat MS, Khabiri SS. Evaluation of vitamin D levels in COVID-19 patients referred to Labafinejad hospital in Tehran and its relationship with disease severity and mortality. Clin Nutr ESPEN 2021;42:313-7.ArticlePubMedPMC
- 21. Murai IH, Fernandes AL, Sales LP, Pinto AJ, Goessler KF, Duran CS, et al. Effect of a single high dose of vitamin D3 on hospital length of stay in patients with moderate to severe COVID-19: a randomized clinical trial. JAMA 2021;325:1053-60.ArticlePubMed
- 22. Infante M, Buoso A, Pieri M, Lupisella S, Nuccetelli M, Bernardin S, et al. Low vitamin d status at admission as a risk factor for poor survival in hospitalized patients with COVID-19: An Italian retrospective study. J Am Coll Nutr 2021;1-16.ArticlePubMed
- 23. Jain A, Chaurasia R, Sengar NS, Singh M, Mahor S, Narain S. Analysis of vitamin D level among asymptomatic and critically ill COVID-19 patients and its correlation with inflammatory markers. Sci Rep 2020;10:20191. ArticlePubMedPMC
- 24. Pinheiro MM, Fabbri A, Infante M. Cytokine storm modulation in COVID-19: a proposed role for vitamin D and DPP-4 inhibitor combination therapy (VIDPP-4i). Immunotherapy 2021;13:753-65.ArticlePubMed
- 25. Malek Mahdavi A. A brief review of interplay between vitamin D and angiotensin-converting enzyme 2: Implications for a potential treatment for COVID-19. Rev Med Virol 2020;30:e2119. PubMedPMC
References
Figure & Data
References
Citations
- The close association of micronutrients with COVID-19
Aimin Zhang, Yue Yin, Jiashu Tian, Xialin Wang, Zhihong Yue, Lin Pei, Li Liu, Li Qin, Mei Jia, Hui Wang, Qingwei Ma, Wei-bo Gao, Lin-Lin Cao
Heliyon.2024; 10(7): e28629. CrossRef - The bounds of meta-analytics and an alternative method
Ramalingam Shanmugam, Mohammad Tabatabai, Derek Wilus, Karan P Singh
Epidemiology and Health.2024; : e2024016. CrossRef - Systematic Mendelian randomization study of the effect of gut microbiome and plasma metabolome on severe COVID-19
Han Yan, Si Zhao, Han-Xue Huang, Pan Xie, Xin-He Cai, Yun-Dan Qu, Wei Zhang, Jian-Quan Luo, Longbo Zhang, Xi Li
Frontiers in Immunology.2023;[Epub] CrossRef - Risk Factors Associated with Severity and Death from COVID-19 in Iran: A Systematic Review and Meta-Analysis Study
Ahmad Mehri, Sahar Sotoodeh Ghorbani, Kosar Farhadi-Babadi, Elham Rahimi, Zahra Barati, Niloufar Taherpour, Neda Izadi, Fatemeh Shahbazi, Yaser Mokhayeri, Arash Seifi, Saeid Fallah, Rezvan Feyzi, Koorosh Etemed, Seyed Saeed Hashemi Nazari
Journal of Intensive Care Medicine.2023; 38(9): 825. CrossRef - Vitamin D: A Role Also in Long COVID-19?
Luigi Barrea, Ludovica Verde, William B. Grant, Evelyn Frias-Toral, Gerardo Sarno, Claudia Vetrani, Florencia Ceriani, Eloisa Garcia-Velasquez, José Contreras-Briceño, Silvia Savastano, Annamaria Colao, Giovanna Muscogiuri
Nutrients.2022; 14(8): 1625. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite