Articles
- Page Path
- HOME > Acute Crit Care > Volume 33(3); 2018 > Article
- Original Article Anti-inflammatory Role of Mesenchymal Stem Cells in an Acute Lung Injury Mouse Model
-
Jin Won Huh1
 , Won Young Kim2, Yun Young Park3, Chae-Man Lim1, Younsuck Koh1, Mi-Jung Kim3, Sang-Bum Hong1
, Won Young Kim2, Yun Young Park3, Chae-Man Lim1, Younsuck Koh1, Mi-Jung Kim3, Sang-Bum Hong1 -
Acute and Critical Care 2018;33(3):154-161.
DOI: https://doi.org/10.4266/acc.2018.00619
Published online: August 31, 2018
1Department of Pulmonary and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
2Department of Emergency Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
3Asan Institute for Life Sciences, Seoul, Korea
- Corresponding author Sang-Bum Hong Department of Pulmonary and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpa-gu, Seoul 05505, Korea Tel: +82-2-3010-3893 Fax: +82-2-3010-6968 E-mail: sbhong@amc.seoul.kr
• Received: December 23, 2017 • Revised: April 6, 2018 • Accepted: July 4, 2018
Copyright © 2018 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background
- Mesenchymal stem cells (MSCs) attenuate injury in various lung injury models through paracrine effects. We hypothesized that intratracheal transplantation of allogenic MSCs could attenuate lipopolysaccharide (LPS)-induced acute lung injury (ALI) in mice, mediated by anti-inflammatory responses.
-
Methods
- Six-week-old male mice were randomized to either the control or the ALI group. ALI was induced by intratracheal LPS instillation. Four hours after LPS instillation, MSCs or phosphate-buffered saline was randomly intratracheally administered. Neutrophil count and protein concentration in bronchoalveolar lavage fluid (BALF); lung histology; levels of interleukin (IL)-1β, IL-6, tumor necrosis factor (TNF)-α, and macrophage inflammatory protein-2; and the expression of proliferation cell nuclear antigen (PCNA), caspase-3, and caspase-9 were evaluated at 48 hours after injury.
-
Results
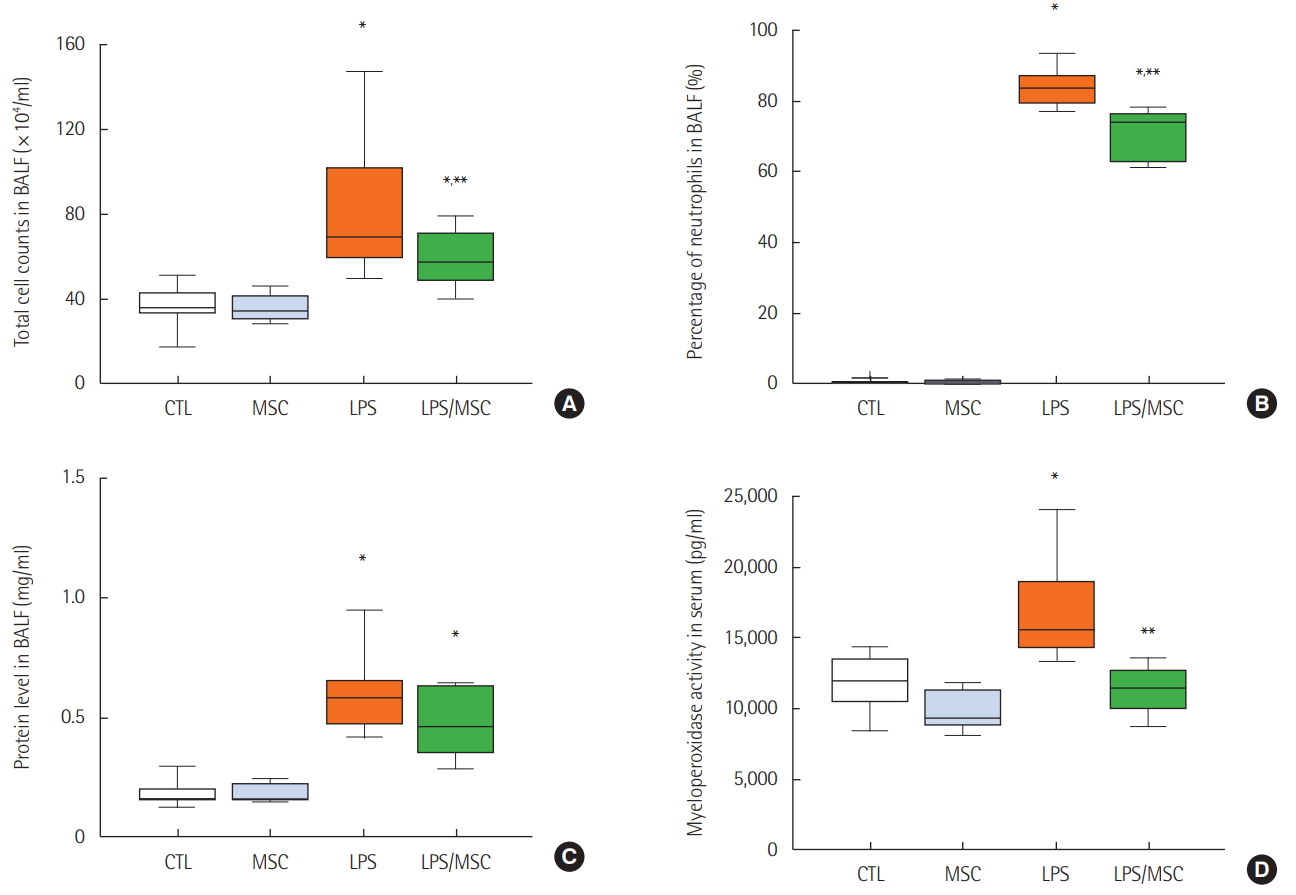
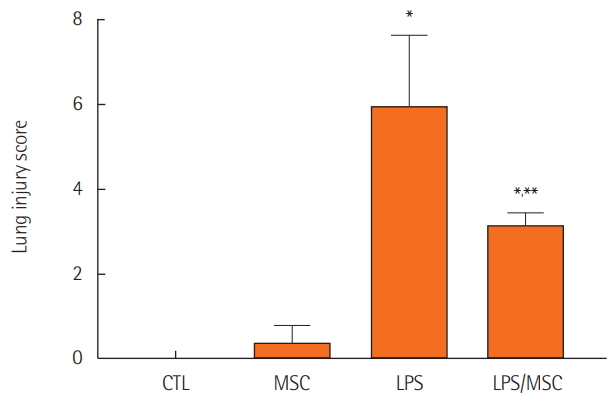
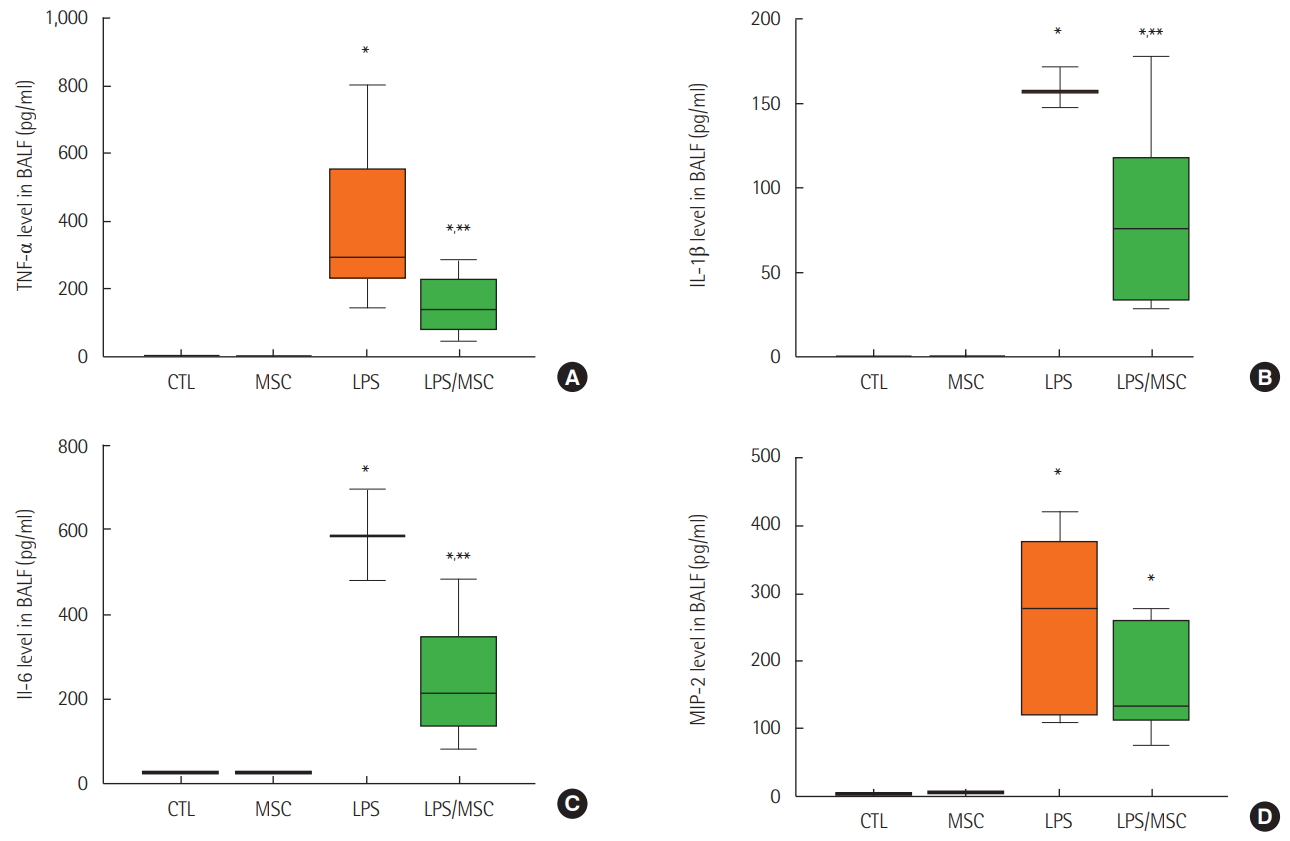
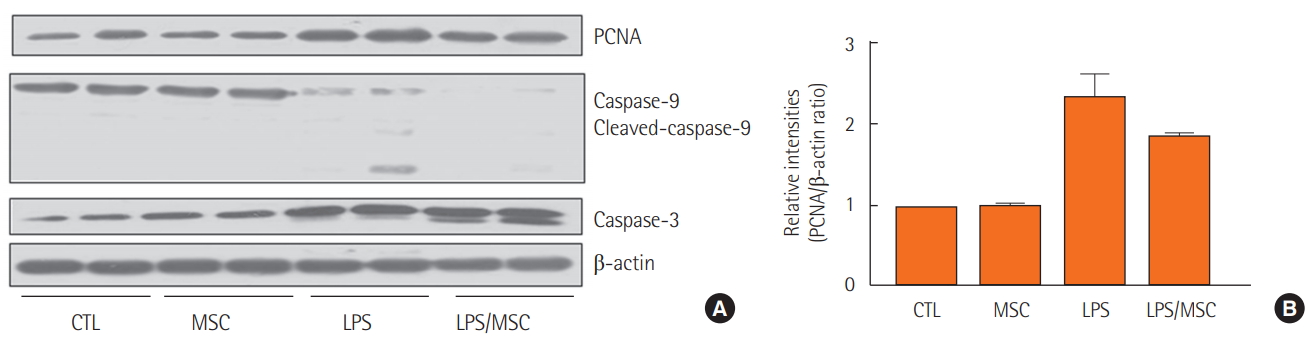
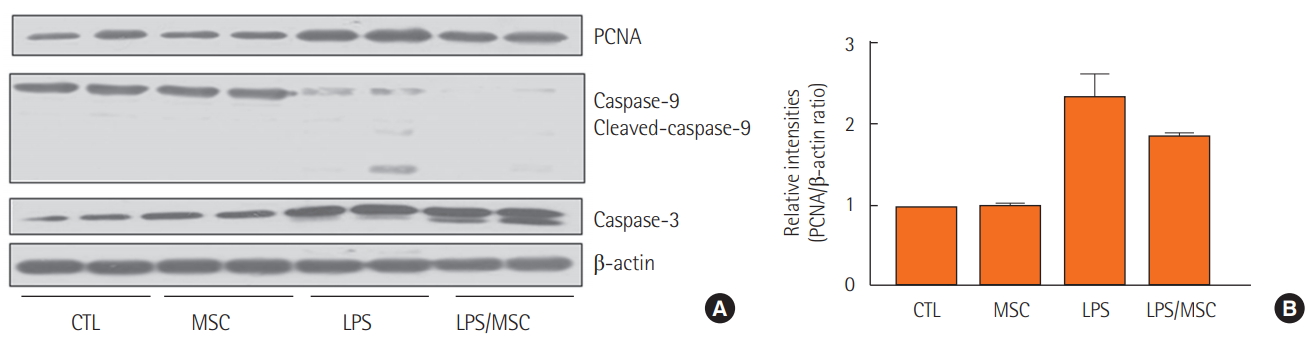
- Treatment with MSCs attenuated lung injury in ALI mice by decreasing protein level and neutrophil recruitment into the BALF and improving the histologic change. MSCs also decreased the protein levels of proinflammatory cytokines including IL-1β, IL-6, and TNF-α, but had little effect on the protein expression of PCNA, caspase-3, and caspase-9.
-
Conclusions
- Intratracheal injection of bone marrow-derived allogenic MSCs attenuates LPS-induced ALI via immunomodulatory effects.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
DISCUSSION
KEY MESSAGES
Acknowledgments
SUPPLEMENTARY MATERIALS
Figure 1.Mesenchymal stem cells attenuate lung injury in lipopolysaccharide-induced acute lung injury. (A) Total cell counts of bronchoalveolar lavage fluid (BALF). (B) Percentage of neutrophils in BALF. (C) Total protein level in BALF. (D) Myeloperoxidase activity in serum. CTL: control group; MSC: mesenchymal stem cell injected group; LPS: lipopolysaccharide-induced acute lung injury group; LPS/MSC: MSC injection following LPS induced acute lung injury group. *P<0.05 compared to the CTL group; **P<0.05 compared to the LPS group.
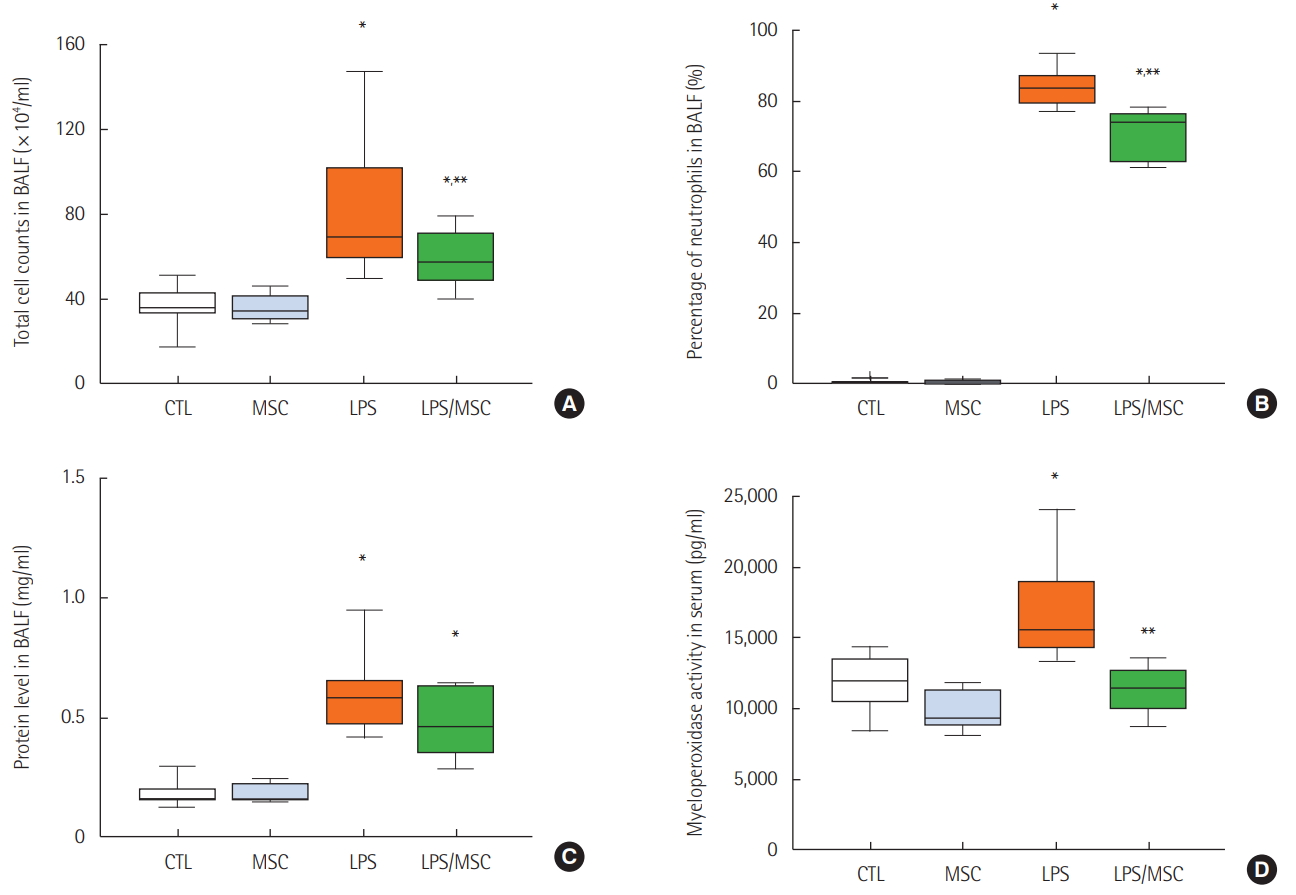
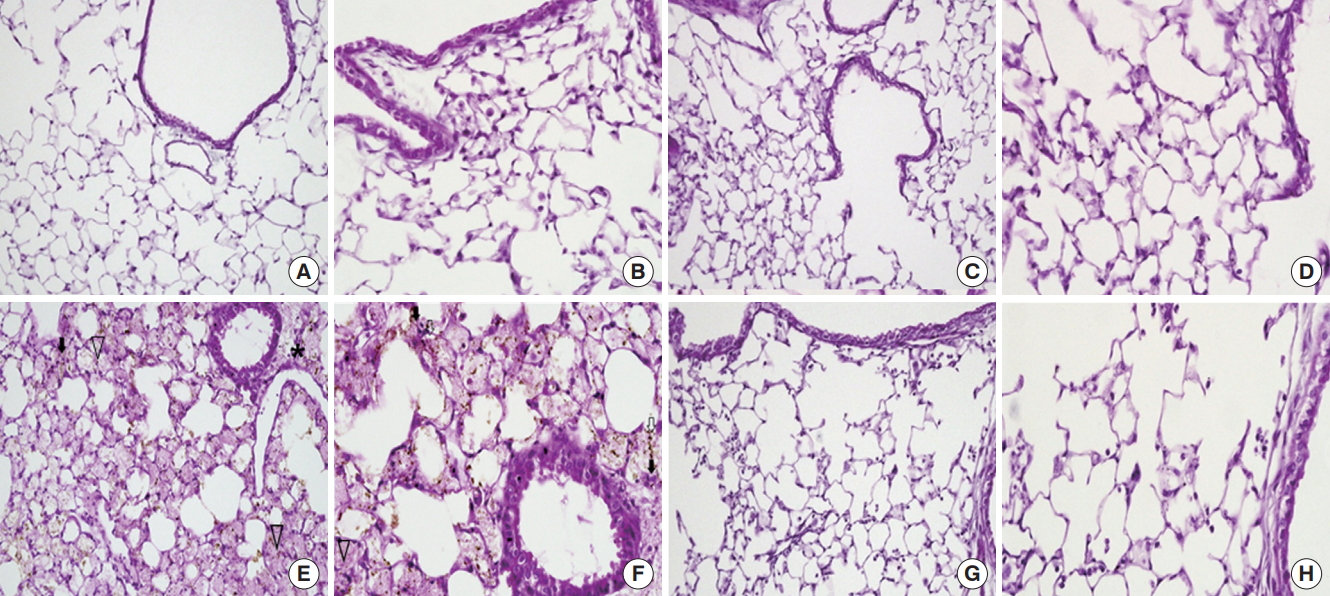
Figure 2.Light microscopy findings of the lung. (A, B) In the control (CTL) group, the normal parenchymal architecture, including the alveolar septa, alveolar lumen, and capillaries were well preserved. The infiltration of inflammatory cells was not observed. (C, D) In the mesenchymal stem cell (MSC) injected group, the normal pulmonary architecture was well preserved similar to that in the CTL group. (E, F) In the lipopolysaccharide (LPS)-induced acute lung injury group, the pulmonary architecture, including the alveolar septa and alveolar lumen were not preserved. Perivascular edema (asterisk) and intrapulmonary hemorrhage (arrow heads) were observed. The infiltration of inflammatory cells, perivascular cuffing (black arrows), and floating of phagocytes in the alveolar lumen (white arrows) were observed. (G, H) In the MSC injection following LPS induced acute lung injury (LPS/MSC) group, the alveolar septa and alveolar lumen were relatively well preserved. Intrapulmonary hemorrhage and perivascular cuffing was less prominent compared to those of the lungs in the LPS group. The infiltration of inflammatory cells was not observed. (H&E; magnification, A, C, E, G: ×200; B, D, F, H: ×400).
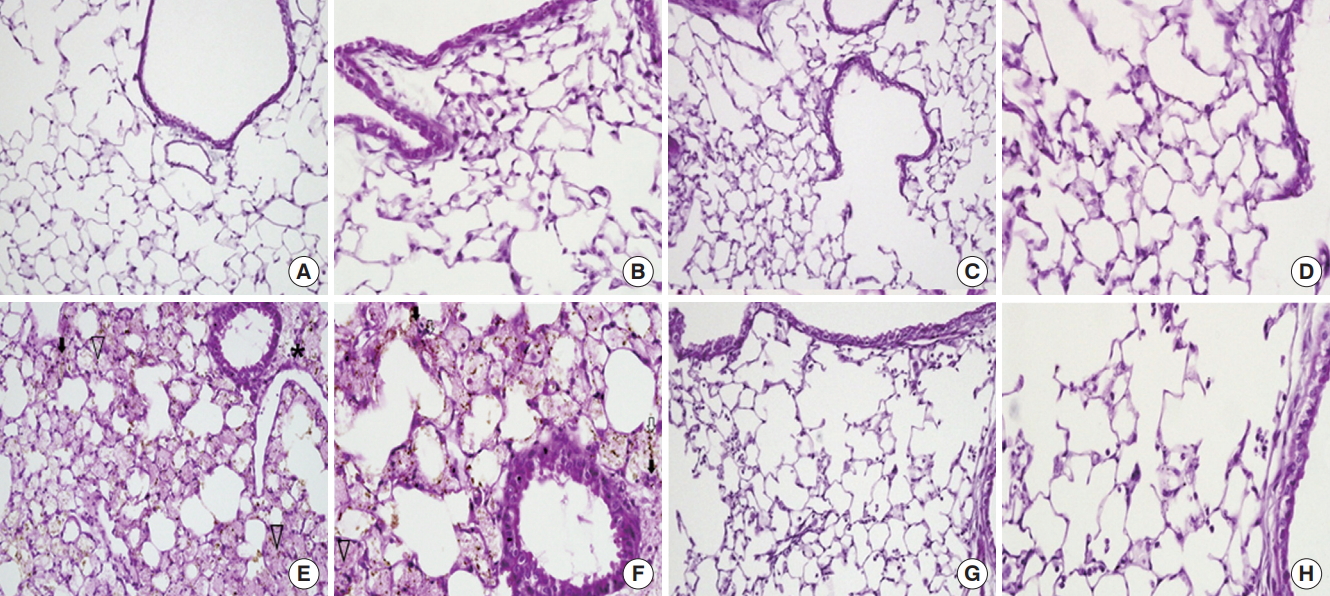
Figure 3.Lung injury scores. CTL: control group; MSC: mesenchymal stem cell injected group; LPS: lipopolysaccharide-induced acute lung injury group; LPS/MSC: MSC injection following LPS induced acute lung injury group. *P<0.05, compared to the CTL group; **P<0.05, compared to the LPS group.
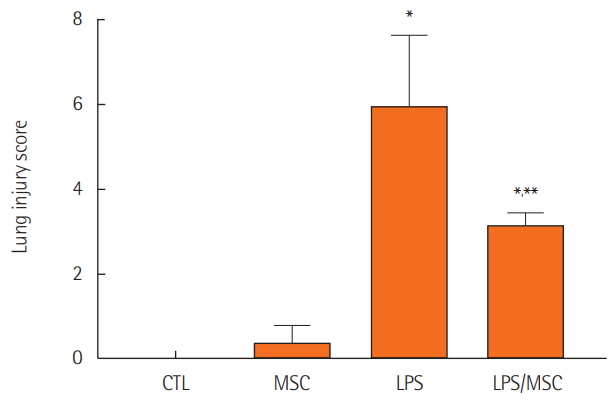
Figure 4.Mesenchymal stem cells attenuate lipopolysaccharide-induced acute lung injury by anti-inflammatory effects. (A) Tumor necrosis factor (TNF)-α, (B) interleukin (IL)-1β, (C) IL-6, and (D) macrophage inflammatory protein (MIP)-2 in bronchoalveolar lavage fluid (BALF). CTL: control group; MSC: mesenchymal stem cell injected group; LPS: lipopolysaccharide-induced acute lung injury group; LPS/MSC: MSC injection following LPS induced acute lung injury group. *P<0.05, compared to the CTL group; **P<0.05, compared to the LPS group.
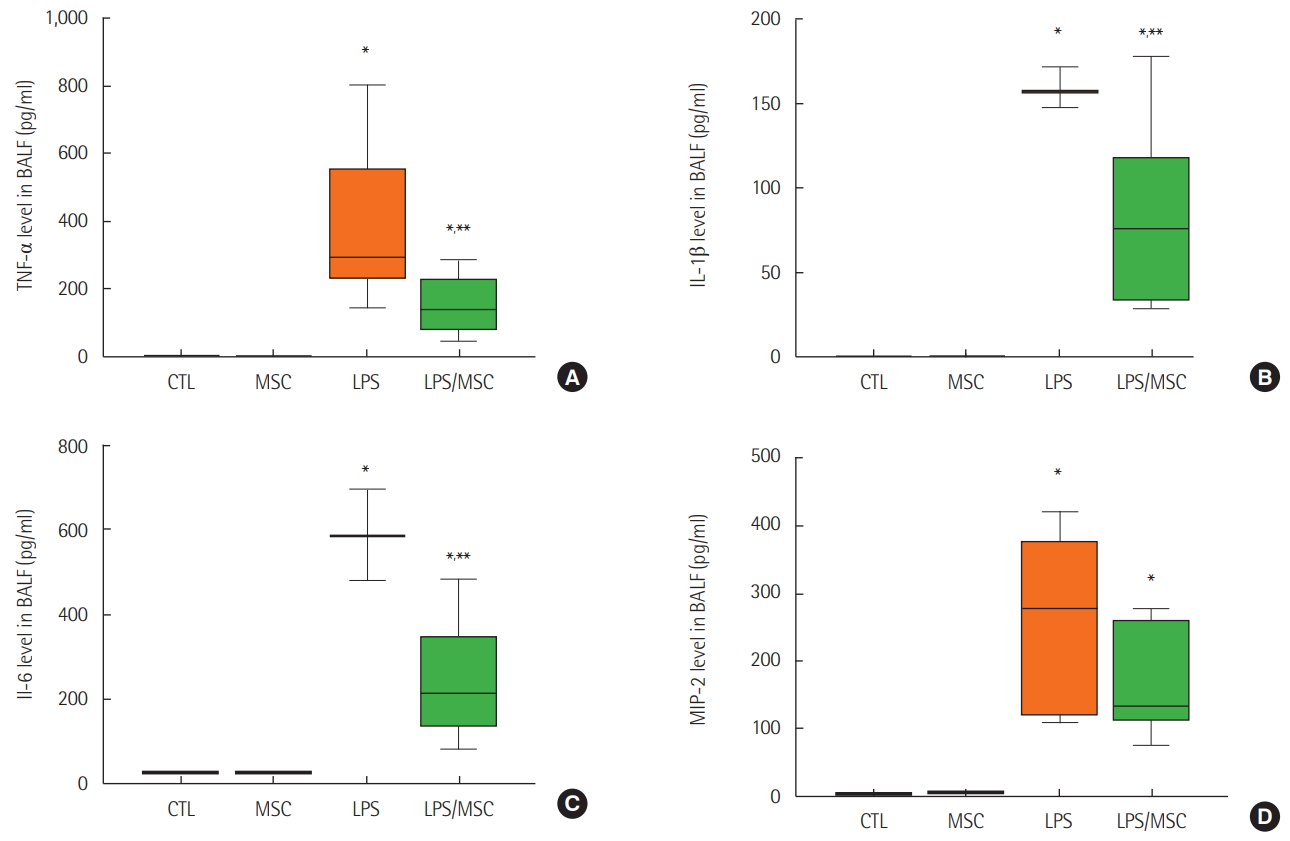
Figure 5.The effect of mesenchymal stem cells on proliferation and cell death. (A) Western blot of proliferation cell nuclear antigen (PCNA), caspase-9 and cleaved-caspase-9, caspase-3, and β-actin. (B) Relative protein level (PCNA/β-actin ratio). CTL: control group; MSC: mesenchymal stem cell injected group; LPS: lipopolysaccharide-induced acute lung injury group; LPS/MSC: MSC injection following LPS induced acute lung injury group.
- 1. Rubenfeld GD, Caldwell E, Peabody E, Weaver J, Martin DP, Neff M, et al. Incidence and outcomes of acute lung injury. N Engl J Med 2005;353:1685-93.ArticlePubMed
- 2. Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA 2016;315:788-800.ArticlePubMed
- 3. Zambon M, Vincent JL. Mortality rates for patients with acute lung injury/ARDS have decreased over time. Chest 2008;133:1120-7.ArticlePubMed
- 4. Amato MB, Barbas CS, Medeiros DM, Magaldi RB, Schettino GP, Lorenzi-Filho G, et al. Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome. N Engl J Med 1998;338:347-54.ArticlePubMed
- 5. Guérin C, Reignier J, Richard JC, Beuret P, Gacouin A, Boulain T, et al. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med 2013;368:2159-68.ArticlePubMed
- 6. Peek GJ, Mugford M, Tiruvoipati R, Wilson A, Allen E, Thalanany MM, et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet 2009;374:1351-63.ArticlePubMed
- 7. Hudson LD, Milberg JA, Anardi D, Maunder RJ. Clinical risks for development of the acute respiratory distress syndrome. Am J Respir Crit Care Med 1995;151:293-301.ArticlePubMed
- 8. Doyle RL, Szaflarski N, Modin GW, Wiener-Kronish JP, Matthay MA. Identification of patients with acute lung injury. Predictors of mortality. Am J Respir Crit Care Med 1995;152:1818-24.ArticlePubMed
- 9. Matthay MA, Zimmerman GA. Acute lung injury and the acute respiratory distress syndrome: four decades of inquiry into pathogenesis and rational management. Am J Respir Cell Mol Biol 2005;33:319-27.ArticlePubMedPMC
- 10. Chollet-Martin S. Polymorphonuclear neutrophil activation during the acute respiratory distress syndrome. Intensive Care Med 2000;26:1575-7.ArticlePubMed
- 11. Abraham E. Neutrophils and acute lung injury. Crit Care Med 2003;31(4 Suppl):S195-9.ArticlePubMed
- 12. Stephens KE, Ishizaka A, Wu ZH, Larrick JW, Raffin TA. Granulocyte depletion prevents tumor necrosis factor-mediated acute lung injury in guinea pigs. Am Rev Respir Dis 1988;138:1300-7.ArticlePubMed
- 13. Perkins GD, Nathani N, McAuley DF, Gao F, Thickett DR. In vitro and in vivo effects of salbutamol on neutrophil function in acute lung injury. Thorax 2007;62:36-42.ArticlePubMed
- 14. Pittenger MF, Mackay AM, Beck SC, Jaiswal RK, Douglas R, Mosca JD, et al. Multilineage potential of adult human mesenchymal stem cells. Science 1999;284:143-7.ArticlePubMed
- 15. Li TS, Hayashi M, Ito H, Furutani A, Murata T, Matsuzaki M, et al. Regeneration of infarcted myocardium by intramyocardial implantation of ex vivo transforming growth factor-betapreprogrammed bone marrow stem cells. Circulation 2005;111:2438-45.ArticlePubMed
- 16. Miyahara Y, Nagaya N, Kataoka M, Yanagawa B, Tanaka K, Hao H, et al. Monolayered mesenchymal stem cells repair scarred myocardium after myocardial infarction. Nat Med 2006;12:459-65.ArticlePubMedPDF
- 17. Lee RH, Pulin AA, Seo MJ, Kota DJ, Ylostalo J, Larson BL, et al. Intravenous hMSCs improve myocardial infarction in mice because cells embolized in lung are activated to secrete the anti-inflammatory protein TSG-6. Cell Stem Cell 2009;5:54-63.ArticlePubMedPMC
- 18. Parekkadan B, van Poll D, Suganuma K, Carter EA, Berthiaume F, Tilles AW, et al. Mesenchymal stem cell-derived molecules reverse fulminant hepatic failure. PLoS One 2007;2:e941.ArticlePubMedPMC
- 19. Mei SH, Haitsma JJ, Dos Santos CC, Deng Y, Lai PF, Slutsky AS, et al. Mesenchymal stem cells reduce inflammation while enhancing bacterial clearance and improving survival in sepsis. Am J Respir Crit Care Med 2010;182:1047-57.ArticlePubMed
- 20. Ortiz LA, Gambelli F, McBride C, Gaupp D, Baddoo M, Kaminski N, et al. Mesenchymal stem cell engraftment in lung is enhanced in response to bleomycin exposure and ameliorates its fibrotic effects. Proc Natl Acad Sci U S A 2003;100:8407-11.ArticlePubMedPMC
- 21. Rojas M, Woods CR, Mora AL, Xu J, Brigham KL. Endotoxininduced lung injury in mice: structural, functional, and biochemical responses. Am J Physiol Lung Cell Mol Physiol 2005;288:L333-41.ArticlePubMed
- 22. Gupta N, Su X, Popov B, Lee JW, Serikov V, Matthay MA. Intrapulmonary delivery of bone marrow-derived mesenchymal stem cells improves survival and attenuates endotoxininduced acute lung injury in mice. J Immunol 2007;179:1855-63.ArticlePubMed
- 23. van Helden HP, Kuijpers WC, Steenvoorden D, Go C, Bruijnzeel PL, van Eijk M, et al. Intratracheal aerosolization of endotoxin (LPS) in the rat: a comprehensive animal model to study adult (acute) respiratory distress syndrome. Exp Lung Res 1997;23:297-316.ArticlePubMed
- 24. Kim ES, Chang YS, Choi SJ, Kim JK, Yoo HS, Ahn SY, et al. Intratracheal transplantation of human umbilical cord bloodderived mesenchymal stem cells attenuates Escherichia coliinduced acute lung injury in mice. Respir Res 2011;12:108. ArticlePubMedPMCPDF
- 25. Dominici M, Le Blanc K, Mueller I, Slaper-Cortenbach I, Marini F, Krause D, et al. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006;8:315-7.ArticlePubMed
- 26. Everhart MB, Han W, Sherrill TP, Arutiunov M, Polosukhin VV, Burke JR, et al. Duration and intensity of NF-kappaB activity determine the severity of endotoxin-induced acute lung injury. J Immunol 2006;176:4995-5005.ArticlePubMed
- 27. Hong SB, Koh Y, Lee IC, Kim MJ, Kim WS, Kim DS, et al. Induced hypothermia as a new approach to lung rest for the acutely injured lung. Crit Care Med 2005;33:2049-55.ArticlePubMed
- 28. Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med 2000;342:1334-49.ArticlePubMed
- 29. Pugin J, Ricou B, Steinberg KP, Suter PM, Martin TR. Proinflammatory activity in bronchoalveolar lavage fluids from patients with ARDS, a prominent role for interleukin-1. Am J Respir Crit Care Med 1996;153:1850-6.ArticlePubMed
- 30. Koh Y, Lee YM, Lim CM, Lee SS, Shim TS, Lee SD, et al. Effects of heat pretreatment on histopathology, cytokine production, and surfactant in endotoxin-induced acute lung injury. Inflammation 2001;25:187-96.ArticlePubMed
- 31. Schütte H, Lohmeyer J, Rosseau S, Ziegler S, Siebert C, Kielisch H, et al. Bronchoalveolar and systemic cytokine profiles in patients with ARDS, severe pneumonia and cardiogenic pulmonary oedema. Eur Respir J 1996;9:1858-67.ArticlePubMed
- 32. Suter PM, Suter S, Girardin E, Roux-Lombard P, Grau GE, Dayer JM. High bronchoalveolar levels of tumor necrosis factor and its inhibitors, interleukin-1, interferon, and elastase, in patients with adult respiratory distress syndrome after trauma, shock, or sepsis. Am Rev Respir Dis 1992;145:1016-22.ArticlePubMed
- 33. Koh Y, Hybertson BM, Jepson EK, Cho OJ, Repine JE. Cytokine-induced neutrophil chemoattractant is necessary for interleukin-1-induced lung leak in rats. J Appl Physiol 1995;79:472-8.ArticlePubMed
- 34. Kawamura H, Kawamura T, Kanda Y, Kobayashi T, Abo T. Extracellular ATP-stimulated macrophages produce macrophage inflammatory protein-2 which is important for neutrophil migration. Immunology 2012;136:448-58.ArticlePubMedPMC
References
Figure & Data
References
Citations
Citations to this article as recorded by 
- The Effectiveness of Adipose Tissue-Derived Mesenchymal Stem Cells Mixed with Platelet-Rich Plasma in the Healing of Inflammatory Bowel Anastomoses: A Pre-Clinical Study in Rats
Georgios Geropoulos, Kyriakos Psarras, Maria Papaioannou, Vasileios Geropoulos, Argyri Niti, Christina Nikolaidou, Georgios Koimtzis, Nikolaos Symeonidis, Efstathios T. Pavlidis, Georgios Koliakos, Theodoros E. Pavlidis, Ioannis Galanis
Journal of Personalized Medicine.2024; 14(1): 121. CrossRef - Cyclic Phytosphingosine-1-Phosphate Primed Mesenchymal Stem Cells Ameliorate LPS-Induced Acute Lung Injury in Mice
Youngheon Park, Jimin Jang, Jooyeon Lee, Hyosin Baek, Jaehyun Park, Sang-Ryul Cha, Se Bi Lee, Sunghun Na, Jae-Woo Kwon, Seok-Ho Hong, Se-Ran Yang
International Journal of Stem Cells.2023; 16(2): 191. CrossRef - Mesenchymal stem cells and their derived exosomes to combat Covid–19
Maryam Yousefi Dehbidi, Nima Goodarzi, Mohammad H. Azhdari, Mohammad Doroudian
Reviews in Medical Virology.2022;[Epub] CrossRef - Stem Cell‐based therapies for COVID‐19‐related acute respiratory distress syndrome
Hoi Wa Ngai, Dae Hong Kim, Mohamed Hammad, Margarita Gutova, Karen Aboody, Christopher D. Cox
Journal of Cellular and Molecular Medicine.2022; 26(9): 2483. CrossRef - Development of a physiomimetic model of acute respiratory distress syndrome by using ECM hydrogels and organ-on-a-chip devices
Esther Marhuenda, Alvaro Villarino, Maria Narciso, Linda Elowsson, Isaac Almendros, Gunilla Westergren-Thorsson, Ramon Farré, Núria Gavara, Jorge Otero
Frontiers in Pharmacology.2022;[Epub] CrossRef - Advances in mesenchymal stromal cell therapy for acute lung injury/acute respiratory distress syndrome
Chang Liu, Kun Xiao, Lixin Xie
Frontiers in Cell and Developmental Biology.2022;[Epub] CrossRef - Auxiliary role of mesenchymal stem cells as regenerative medicine soldiers to attenuate inflammatory processes of severe acute respiratory infections caused by COVID-19
Peyvand Parhizkar Roudsari, Sepideh Alavi-Moghadam, Moloud Payab, Forough Azam Sayahpour, Hamid Reza Aghayan, Parisa Goodarzi, Fereshteh Mohamadi-jahani, Bagher Larijani, Babak Arjmand
Cell and Tissue Banking.2020; 21(3): 405. CrossRef - The Role of MSC Therapy in Attenuating the Damaging Effects of the Cytokine Storm Induced by COVID-19 on the Heart and Cardiovascular System
Georgina M. Ellison-Hughes, Liam Colley, Katie A. O'Brien, Kirsty A. Roberts, Thomas A. Agbaedeng, Mark D. Ross
Frontiers in Cardiovascular Medicine.2020;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite