Articles
- Page Path
- HOME > Acute Crit Care > Volume 34(2); 2019 > Article
-
Case Report
Cardiology Acute fulminant myocarditis following influenza vaccination requiring extracorporeal membrane oxygenation -
Youn-Jung Kim
 , Jun-Il Bae, Seung Mok Ryoo, Won Young Kim
, Jun-Il Bae, Seung Mok Ryoo, Won Young Kim -
Acute and Critical Care 2018;34(2):165-169.
DOI: https://doi.org/10.4266/acc.2017.00045
Published online: November 7, 2018
Department of Emergency Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- Corresponding author Won Young Kim Department of Emergency Medicine, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpa-gu, Seoul 05505, Korea Tel: +82-2-3010-3350 Fax: +82-2-3010-3360 E-mail: wonpia73@naver.com
• Received: January 25, 2017 • Revised: April 29, 2017 • Accepted: May 2, 2017
Copyright © 2019 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
- The inactivated influenza vaccination is generally safe with mostly mild side effects. We report a rare but fatal adverse event following influenza vaccination. A previously healthy 27-year-old woman who received the influenza vaccination 3 days before presenting to the emergency department had rapidly aggravating dyspnea and mental deterioration. She was diagnosed as having acute fulminant myocarditis with refractory cardiogenic shock, which was successfully managed with veno-arterial extracorporeal membrane oxygenation. The cardiac function of the patient recovered in 3 weeks.
CASE REPORT
DISCUSSION
Figure 1.Serial changes of vital signs and lactic acid level for 10 hours after emergency department (ED) presentation. ECMO: extracorporeal membrane oxygenation; ICU: intensive care unit.

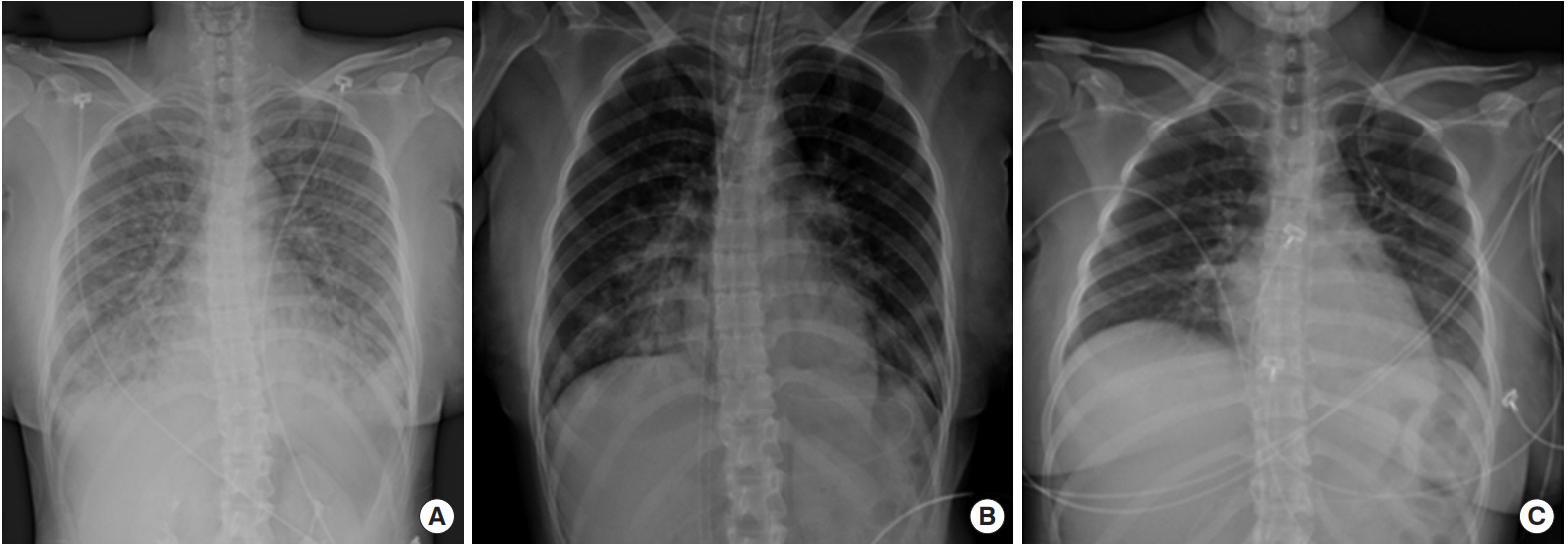
Figure 2.Serial chest X-rays during hospitalization. (A) Chest X-ray showed diffuse ground glass opacities on both lung fields at 4 hours after emergency department presentation. (B) Chest X-ray after insertion of extracorporeal membrane oxygenation and intubation at emergency department. (C) Chest X-ray after recovery on the 9th day of hospitalization.

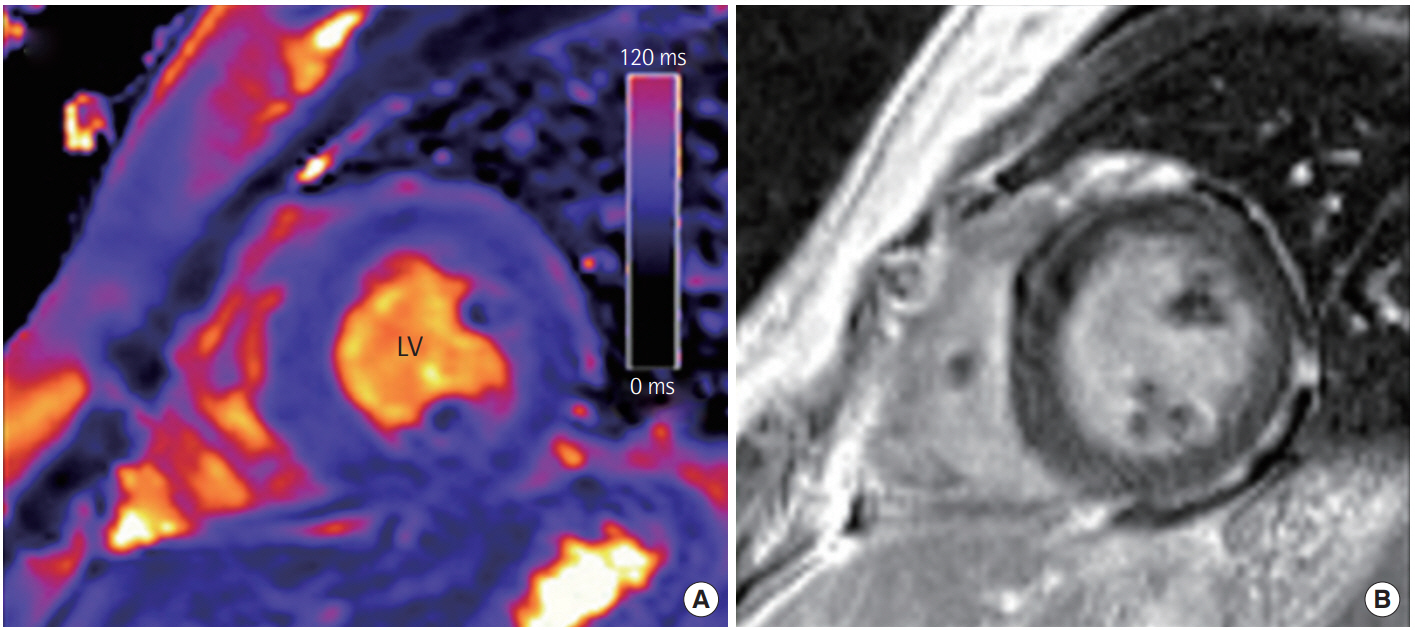
Figure 3.Representative cardiovascular magnetic resonance findings in a patient with acute myocarditis. (A) Short-axis T2 map revealed an increased global myocardial T2 value of 68–72 ms in this patient. (B) Late gadolinium enhancement shows mild diffuse midwall enhancement in the left ventricular (LV) myocardium.
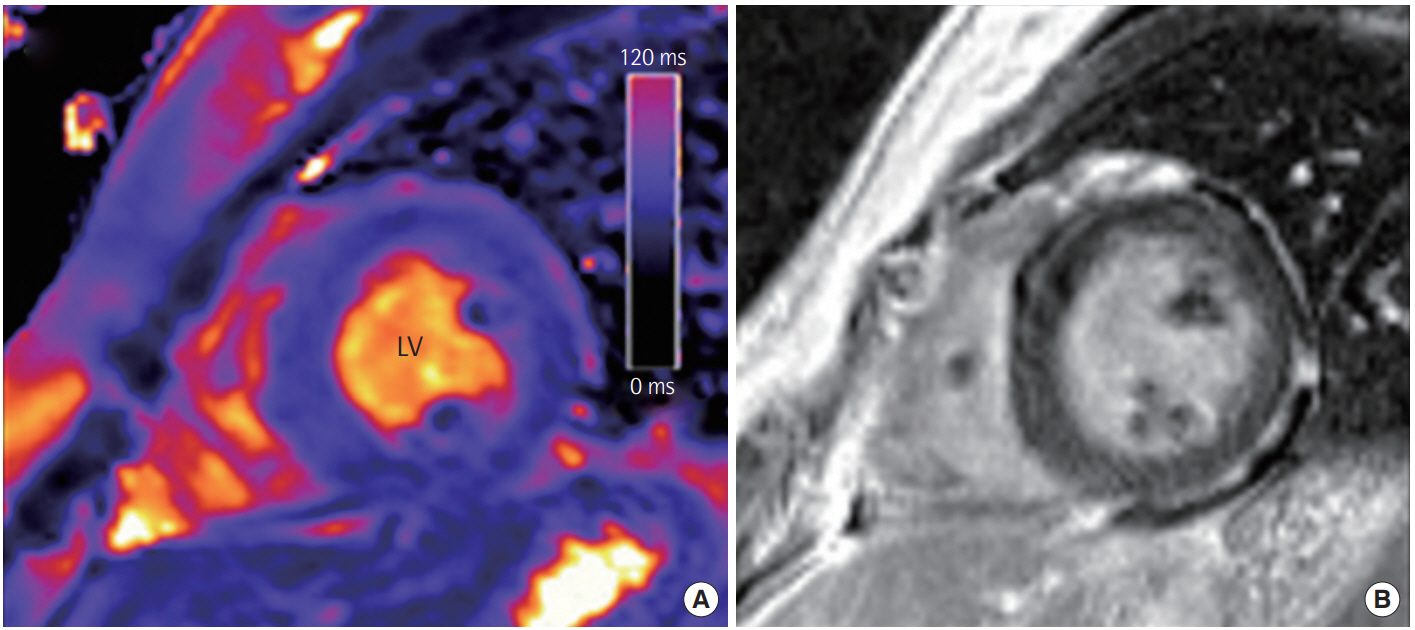
Table 1.Serial changes of laboratory findings
- 1. Korea Centers for Disease Control and Prevention. Korea Centers for Disease Control and Prevention (KCDC) web [Internet]. Cheongju, Korea Centers for Disease Control and Prevention. 2017;[cited 2017 Oct 19]. Available from: http://cdc.go.kr/CDC/mobile/intro/CdcKrIntro0505.jsp?menuIds=HOME001-MNU1154-MNU2557-MNU2487&cid=76303.
- 2. Nichol KL, Margolis KL, Lind A, Murdoch M, Mc-Fadden R, Hauge M, et al. Side effects associated with influenza vaccination in healthy working adults: a randomized, placebocontrolled trial. Arch Intern Med 1996;156:1546-50.ArticlePubMed
- 3. de Meester A, Luwaert R, Chaudron JM. Symptomatic pericarditis after influenza vaccination: report of two cases. Chest 2000;117:1803-5.ArticlePubMed
- 4. Cheng MP, Kozoriz MG, Ahmadi AA, Kelsall J, Paquette K, Onrot JM. Post-vaccination myositis and myocarditis in a previously healthy male. Allergy Asthma Clin Immunol 2016;12:6. ArticlePubMedPMC
- 5. Singh K, Marinelli T, Horowitz JD. Takotsubo cardiomyopathy after anti-influenza vaccination: catecholaminergic effects of immune system. Am J Emerg Med 2013;31:1627. e1-4.Article
- 6. Streifler JJ, Dux S, Garty M, Rosenfeld JB. Recurrent pericarditis: a rare complication of influenza vaccination. Br Med J (Clin Res Ed) 1981;283:526-7.Article
- 7. Rosenberg M, Sparks R, McMahon A, Iskander J, Campbell JD, Edwards KM. Serious adverse events rarely reported after trivalent inactivated influenza vaccine (TIV) in children 6-23 months of age. Vaccine 2009;27:4278-83.ArticlePubMed
- 8. Lanza GA, Barone L, Scalone G, Pitocco D, Sgueglia GA, Mollo R, et al. Inflammation-related effects of adjuvant influenza A vaccination on platelet activation and cardiac autonomic function. J Intern Med 2011;269:118-25.ArticlePubMed
- 9. Engler RJ, Nelson MR, Collins LC Jr, Spooner C, Hemann BA, Gibbs BT, et al. A prospective study of the incidence of myocarditis/pericarditis and new onset cardiac symptoms following smallpox and influenza vaccination. PLoS One 2015;10:e0118283. ArticlePubMedPMC
References
Figure & Data
References
Citations
Citations to this article as recorded by 
- Clinical Characteristics and Mechanisms of Acute Myocarditis
Stephane Heymans, Sophie Van Linthout, Sarah Mignon Kraus, Leslie T. Cooper, Ntobeko A.B. Ntusi
Circulation Research.2024; 135(2): 397. CrossRef - Active surveillance for adverse events of influenza vaccine safety in elderly cancer patients using self-controlled tree-temporal scan statistic analysis
Na-Young Jeong, Chung-Jong Kim, Sang Min Park, Ye-Jee Kim, Joongyub Lee, Nam-Kyong Choi
Scientific Reports.2023;[Epub] CrossRef - The Incidence of Myocarditis Following an Influenza Vaccination: A Population-Based Observational Study
Wen-Hwa Wang, Kai-Che Wei, Yu-Tung Huang, Kuang-Hua Huang, Tung-Han Tsai, Yu-Chia Chang
Drugs & Aging.2023; 40(2): 145. CrossRef - Comparison of COVID-19 Vaccine-Associated Myocarditis and Viral Myocarditis Pathology
Kamron Reza Hamedi, Gannett Loftus, Lawson Traylor, Richard Goodwin, Sergio Arce
Vaccines.2023; 11(2): 362. CrossRef - Myocarditis and autoimmunity
Akira Matsumori
Expert Review of Cardiovascular Therapy.2023; 21(6): 437. CrossRef - Cardiovascular magnetic resonance (CMR) and positron emission tomography (PET) imaging in the diagnosis and follow-up of patients with acute myocarditis and chronic inflammatory cardiomyopathy
Federico Caobelli, Jordi Broncano Cabrero, Nicola Galea, Philip Haaf, Christian Loewe, Julian A. Luetkens, Giuseppe Muscogiuri, Marco Francone
The International Journal of Cardiovascular Imaging.2023; 39(11): 2221. CrossRef - Clinical Syndromes Related to SARS-CoV-2 Infection and Vaccination in Pediatric Age: A Narrative Review
Maria Vincenza Mastrolia, Camilla De Cillia, Michela Orlandi, Sarah Abu-Rumeileh, Ilaria Maccora, Valerio Maniscalco, Edoardo Marrani, Ilaria Pagnini, Gabriele Simonini
Medicina.2023; 59(11): 2027. CrossRef - Acute Lymphocyte Myocarditis Associated with Influenza Vaccination
Ryo Nakamura, Shin-ichi Ando, Seiya Kato, Toshiaki Kadokami
Internal Medicine.2022; 61(15): 2307. CrossRef - Clinically Suspected Myocarditis Temporally Related to COVID-19 Vaccination in Adolescents and Young Adults: Suspected Myocarditis After COVID-19 Vaccination
Dongngan T. Truong, Audrey Dionne, Juan Carlos Muniz, Kimberly E. McHugh, Michael A. Portman, Linda M. Lambert, Deepika Thacker, Matthew D. Elias, Jennifer S. Li, Olga H. Toro-Salazar, Brett R. Anderson, Andrew M. Atz, C. Monique Bohun, M. Jay Campbell, M
Circulation.2022; 145(5): 345. CrossRef - Myocarditis following rAd26 and rAd5 vector‐based COVID‐19 vaccine: case report
Farah Naghashzadeh, Shadi Shafaghi, Atosa Dorudinia, Seyed Alireza Naji, Majid Marjani, Ahmad Amin, Arezoo Mohamadifar, Sima Noorali, Babak Sharif Kashani
ESC Heart Failure.2022; 9(2): 1483. CrossRef - Myocarditis following COVID-19 vaccination in adolescents and adults: a cumulative experience of 2021
Onyedika J. Ilonze, Maya E. Guglin
Heart Failure Reviews.2022; 27(6): 2033. CrossRef - Chest Pain and Suspected Myocarditis Related to COVID-19 Vaccination in Adolescents—A Case Series
Da-Eun Roh, Hyejin Na, Jung-Eun Kwon, Insu Choi, Yeo-Hyang Kim, Hwa-Jin Cho
Children.2022; 9(5): 693. CrossRef - Cardiac Adverse Events after Vaccination—A Systematic Review
Kanak Parmar, Sai Subramanyam, Gaspar Del Rio-Pertuz, Pooja Sethi, Erwin Argueta-Sosa
Vaccines.2022; 10(5): 700. CrossRef - A case of myocarditis after COVID-19 vaccination: incidental or consequential?
Leona S. Alizadeh, Vitali Koch, Ibrahim Yel, Leon D. Grünewald, Daniel Mathies, Simon Martin, Thomas J. Vogl, Dominic Rauschning, Christian Booz
Heliyon.2022; 8(6): e09537. CrossRef - COVID-19 Vaccination and the Rate of Immune and Autoimmune Adverse Events Following Immunization: Insights From a Narrative Literature Review
Naim Mahroum, Noy Lavine, Aviran Ohayon, Ravend Seida, Abdulkarim Alwani, Mahmoud Alrais, Magdi Zoubi, Nicola Luigi Bragazzi
Frontiers in Immunology.2022;[Epub] CrossRef - COVID-19 vaccination and carditis in children and adolescents: a systematic review and meta-analysis
Oscar Hou In Chou, Jonathan Mui, Cheuk To Chung, Danny Radford, Simon Ranjithkumar, Endurance Evbayekha, Ronald Nam, Levent Pay, Danish Iltaf Satti, Sebastian Garcia-Zamora, George Bazoukis, Göksel Çinier, Sharen Lee, Vassilios S. Vassiliou, Tong Liu, Gar
Clinical Research in Cardiology.2022; 111(10): 1161. CrossRef - Myopericarditis after vaccination, Vaccine Adverse Event Reporting System (VAERS), 1990–2018
John R. Su, Michael M. McNeil, Kerry J. Welsh, Paige L. Marquez, Carmen Ng, Ming Yan, Maria V. Cano
Vaccine.2021; 39(5): 839. CrossRef - Sipuleucel‐T associated inflammatory cardiomyopathy: a case report and observations from a large pharmacovigilance database
Melissa Y.Y. Moey, Rahim A. Jiwani, Kotaro Takeda, Karyn Prenshaw, R. Wayne Kreeger, John Inzerillo, Darla K. Liles, C. Bogdan Marcu, Bénédicte Lebrun‐Vignes, D. Lynn Morris, Sivakumar Ardhanari, Joe‐Elie Salem
ESC Heart Failure.2021; 8(4): 3360. CrossRef - Myocarditis following COVID-19 vaccination
Elisabeth Albert, Gerard Aurigemma, Jason Saucedo, David S. Gerson
Radiology Case Reports.2021; 16(8): 2142. CrossRef - Myocarditis and Other Cardiovascular Complications of the mRNA-Based COVID-19 Vaccines
Mahesh K Vidula, Marietta Ambrose, Helene Glassberg, Neel Chokshi, Tiffany Chen, Victor A Ferrari, Yuchi Han
Cureus.2021;[Epub] CrossRef - Patients With Acute Myocarditis Following mRNA COVID-19 Vaccination
Han W. Kim, Elizabeth R. Jenista, David C. Wendell, Clerio F. Azevedo, Michael J. Campbell, Stephen N. Darty, Michele A. Parker, Raymond J. Kim
JAMA Cardiology.2021; 6(10): 1196. CrossRef - Acute myocarditis following Comirnaty vaccination in a healthy man with previous SARS-CoV-2 infection
Anna Patrignani, Nicolò Schicchi, Francesca Calcagnoli, Elena Falchetti, Nino Ciampani, Giulio Argalia, Antonio Mariani
Radiology Case Reports.2021; 16(11): 3321. CrossRef - Myocarditis and pericarditis after vaccination for COVID‐19
Blake Hudson, Ryan Mantooth, Matthew DeLaney
Journal of the American College of Emergency Physicians Open.2021;[Epub] CrossRef - Myocarditis, Pericarditis and Cardiomyopathy After COVID-19 Vaccination
Salvatore Pepe, Ann T. Gregory, A. Robert Denniss
Heart, Lung and Circulation.2021; 30(10): 1425. CrossRef - Cardiac Manifestations of Multisystem Inflammatory Syndrome in Children (MIS-C) Following COVID-19
Eveline Y. Wu, M. Jay Campbell
Current Cardiology Reports.2021;[Epub] CrossRef - Hemodynamic Collapse After Influenza Vaccination: A Vaccine-Induced Fulminant Myocarditis?
Nobutaka Nagano, Toshiyuki Yano, Yugo Fujita, Masayuki Koyama, Ryo Hasegawa, Jun Nakata, Ryo Nishikawa, Naoto Murakami, Takefumi Fujito, Atsushi Mochizuki, Hidemichi Kouzu, Atsuko Muranaka, Nobuaki Kokubu, Tetsuji Miura
Canadian Journal of Cardiology.2020; 36(9): 1554.e5. CrossRef - Fatal influenza myocarditis with incessant ventricular tachycardia
Nidhi Saraiya, Supriya Singh, Marilou Corpuz
BMJ Case Reports.2019; 12(7): e228201. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite