
Articles
- Page Path
- HOME > Acute Crit Care > Volume 36(3); 2021 > Article
-
Original Article
Pulmonary Effects of high-flow nasal cannula in patients with mild to moderate hypercapnia: a prospective observational study -
Kyung Hun Nam1
 , Hyung Koo Kang2, Sung-Soon Lee2, So-Hee Park2, Sung Wook Kang3, Jea Jun Hwang3, So Young Park4, Won Young Kim5, Hee Jung Suh6, Eun Young Kim6, Ga Jin Seo6, Younsuck Koh7, Sang-Bum Hong7, Jin Won Huh7, Chae-Man Lim7
, Hyung Koo Kang2, Sung-Soon Lee2, So-Hee Park2, Sung Wook Kang3, Jea Jun Hwang3, So Young Park4, Won Young Kim5, Hee Jung Suh6, Eun Young Kim6, Ga Jin Seo6, Younsuck Koh7, Sang-Bum Hong7, Jin Won Huh7, Chae-Man Lim7 -
Acute and Critical Care 2021;36(3):249-255.
DOI: https://doi.org/10.4266/acc.2020.01102
Published online: July 26, 2021
1Department of Medicine, Ajou University Intermediate Care Hospital, Suwon, Korea
2Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Inje University Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea
3Department of Pulmonary and Critical Care Medicine, Kyung Hee University Hospital at Gangdong, Seoul, Korea
4Department of Pulmonology, Ewha Womans University Seoul Hospital, Seoul, Korea
5Department of Emergency Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
6Intensive Care Nursing Team, Asan Medical Center, Seoul, Korea
7Department of Pulmonary and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- Corresponding author Chae-Man Lim Department of Pulmonary and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpa-gu, Seoul 05505, Korea Tel: +82-2-3010-4700 Fax: +82-2-2045-4039 E-mail: cmlim@amc.seoul.kr
- *Current affiliation: Department of Critical Care Medicine, Seongnam Citizens Medical Center, Seongnam, Korea
Copyright © 2021 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background
- Evidence for using high-flow nasal cannula (HFNC) in hypercapnia is still limited. Most of the clinical studies had been conducted retrospectively, and there had been conflicting reports for the effects of HFNC on hypercapnia correction in prospective studies. Therefore, more evidence is needed to understand the effect of the HFNC in hypercapnia.
-
Methods
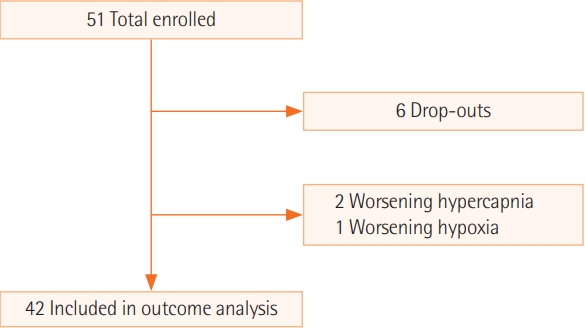
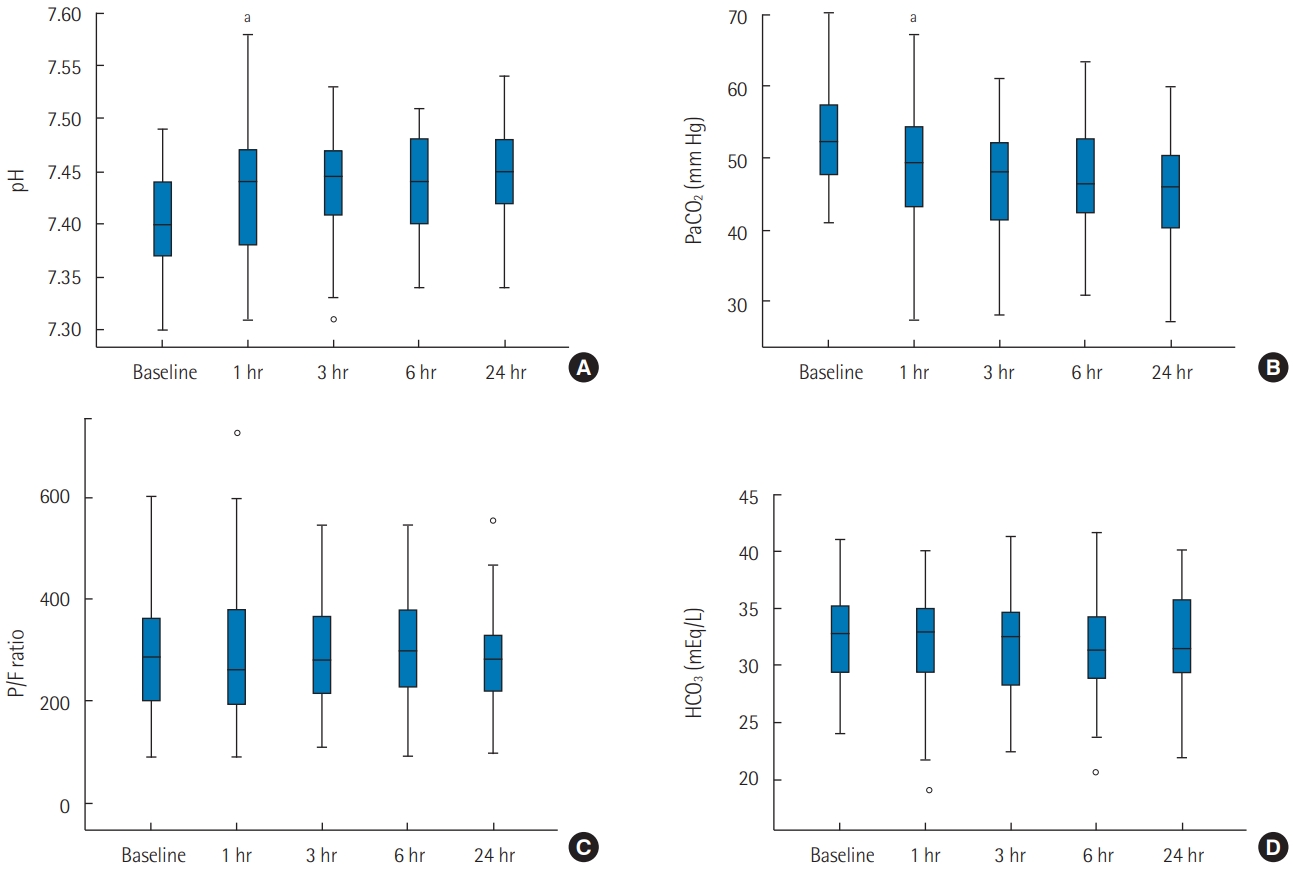
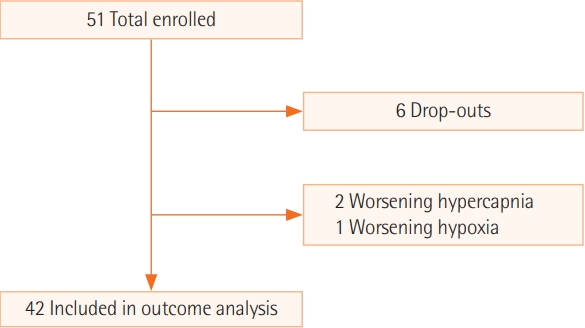
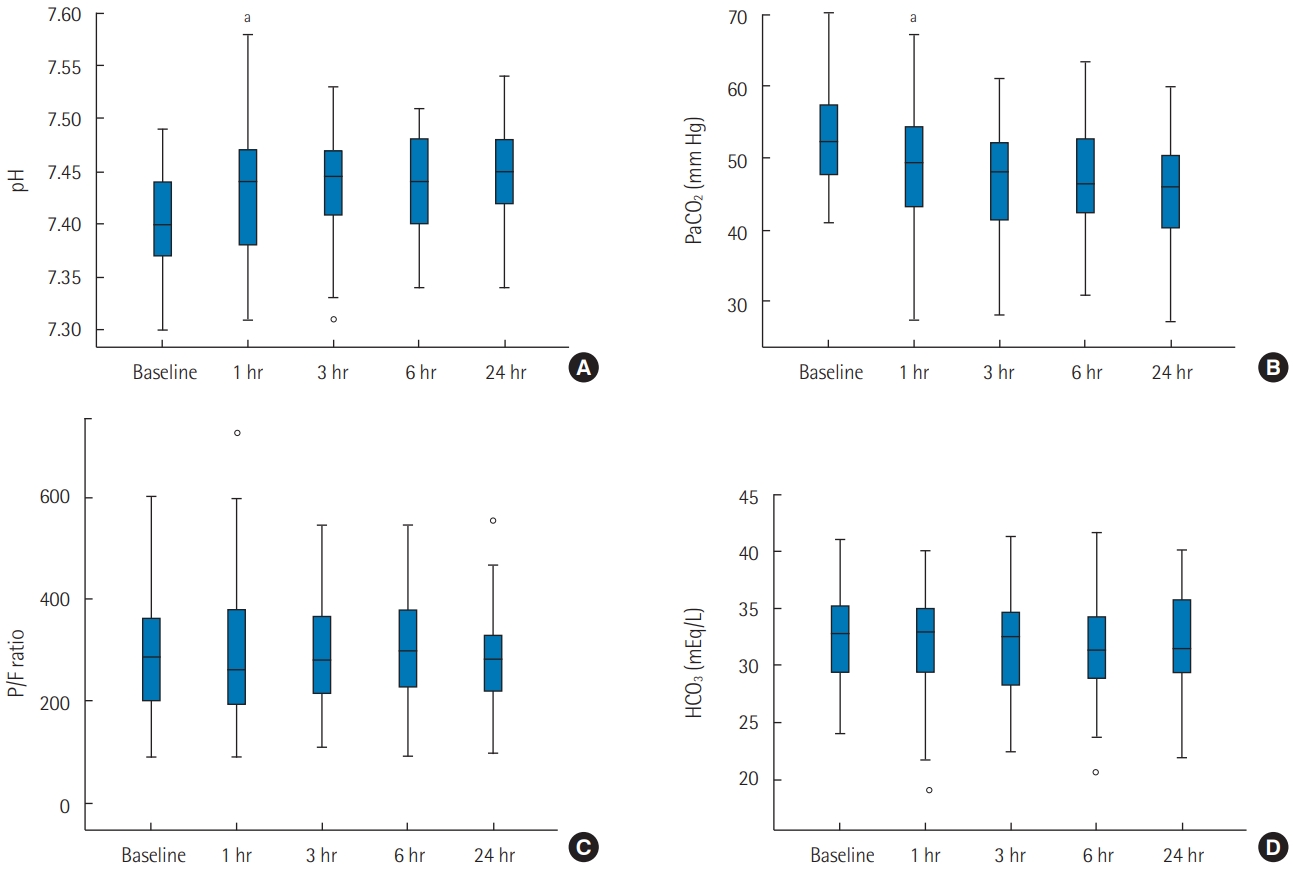
- We conducted a multicenter prospective observational study after applying HFNC to 45 hospitalized subjects who had moderate hypercapnia (arterial partial pressure of carbon dioxide [PaCO2], 43–70 mm Hg) without severe respiratory acidosis (pH <7.30). The primary outcome was a change in PaCO2 level in the first 24 hours of HFNC use. The secondary outcomes were changes in other parameters of arterial blood gas analysis, changes in respiration rates, and clinical outcomes.
-
Results
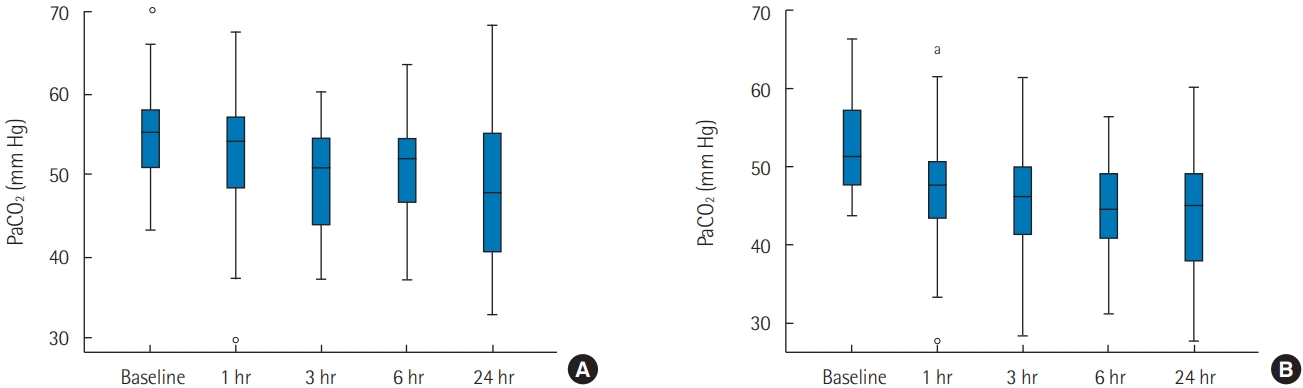
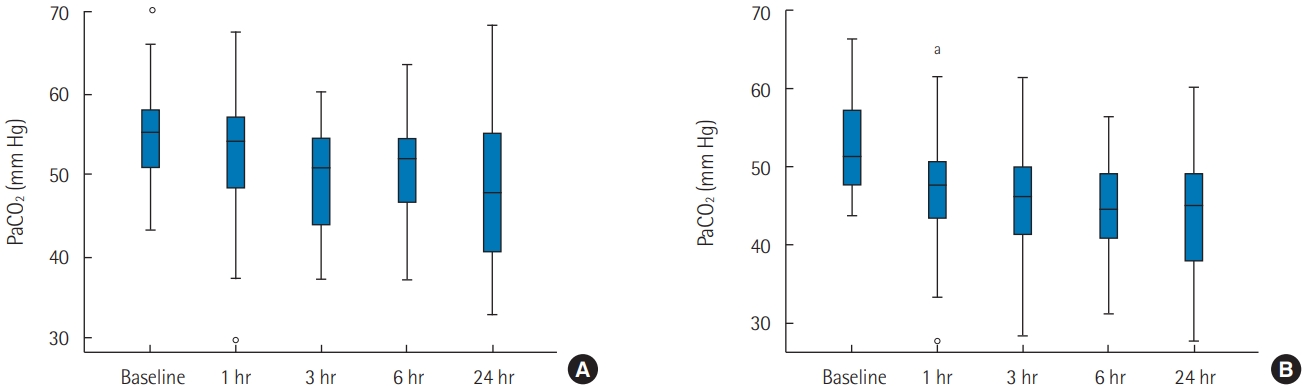
- There was a significant decrease in PaCO2 in the first hour of HFNC application (-3.80 mm Hg; 95% confidence interval, -6.35 to -1.24; P<0.001). Reduction of PaCO2 was more prominent in subjects who did not have underlying obstructive lung disease. There was a correction in pH, but no significant changes in respiratory rate, bicarbonate, and arterial partial pressure of oxygen/fraction of inspired oxygen ratio. Mechanical ventilation was not required for 93.3% (42/45) of our study population.
-
Conclusions
- We suggest that HFNC could be a safe alternative for oxygen delivery in hypercapnia patients who do not need immediate mechanical ventilation. With HFNC oxygenation, correction of hypercapnia could be expected, especially in patients who do not have obstructive lung diseases.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
PaCO2 changes in the obstructive and non-obstructive groups
DISCUSSION
KEY MESSAGES
-
CONFLICT OF INTEREST No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conceptualization: KHN, WYK, CML. Data curation: KHN, HJS, EYK, GJS. Formal analysis: KHN. Funding acquisition: CML. Methodology: all authors. Project administration: CML, KHN. Investigation: all authors. Visualization: KHN. Writing–original draft: KHN. Writing–review & editing: CML.
NOTES
Acknowledgments
- 1. Drake MG. High-flow nasal cannula oxygen in adults: an evidence-based assessment. Ann Am Thorac Soc 2018;15:145-55.ArticlePubMed
- 2. Möller W, Celik G, Feng S, Bartenstein P, Meyer G, Oliver E, et al. Nasal high flow clears anatomical dead space in upper airway models. J Appl Physiol (1985) 2015;118:1525-32.ArticlePubMedPMC
- 3. Bräunlich J, Goldner F, Wirtz H. Nasal highflow eliminates CO2 from lower airways. Respir Physiol Neurobiol 2017;242:86-8.ArticlePubMed
- 4. Biselli PJ, Kirkness JP, Grote L, Fricke K, Schwartz AR, Smith P, et al. Nasal high-flow therapy reduces work of breathing compared with oxygen during sleep in COPD and smoking controls: a prospective observational study. J Appl Physiol (1985) 2017;122:82-8.ArticlePubMed
- 5. Patel A, Nouraei SA. Transnasal humidified rapid-insufflation ventilatory exchange (THRIVE): a physiological method of increasing apnoea time in patients with difficult airways. Anaesthesia 2015;70:323-9.ArticlePubMed
- 6. Jeong JH, Kim DH, Kim SC, Kang C, Lee SH, Kang TS, et al. Changes in arterial blood gases after use of high-flow nasal cannula therapy in the ED. Am J Emerg Med 2015;33:1344-9.ArticlePubMed
- 7. Kim ES, Lee H, Kim SJ, Park J, Lee YJ, Park JS, et al. Effectiveness of high-flow nasal cannula oxygen therapy for acute respiratory failure with hypercapnia. J Thorac Dis 2018;10:882-8.ArticlePubMedPMC
- 8. Sztrymf B, Messika J, Mayot T, Lenglet H, Dreyfuss D, Ricard JD. Impact of high-flow nasal cannula oxygen therapy on intensive care unit patients with acute respiratory failure: a prospective observational study. J Crit Care 2012;27:324.e9-13.ArticlePubMed
- 9. Frat JP, Thille AW, Mercat A, Girault C, Ragot S, Perbet S, et al. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N Engl J Med 2015;372:2185-96.ArticlePubMed
- 10. Rochwerg B, Granton D, Wang DX, Helviz Y, Einav S, Frat JP, et al. High flow nasal cannula compared with conventional oxygen therapy for acute hypoxemic respiratory failure: a systematic review and meta-analysis. Intensive Care Med 2019;45:563-72.ArticlePubMed
- 11. Nilius G, Franke KJ, Domanski U, Rühle KH, Kirkness JP, Schneider H. Effects of nasal insufflation on arterial gas exchange and breathing pattern in patients with chronic obstructive pulmonary disease and hypercapnic respiratory failure. Adv Exp Med Biol 2013;755:27-34.ArticlePubMed
- 12. Roussos C, Koutsoukou A. Respiratory failure. Eur Respir J Suppl 2003;47:3s-14s.ArticlePubMed
- 13. Davidson AC, Banham S, Elliott M, Kennedy D, Gelder C, Glossop A. BTS/ICS guideline for the ventilatory management of acute hypercapnic respiratory failure in adults. Thorax 2016;71 Suppl 2:ii1-35.ArticlePubMed
- 14. Papachatzakis Y, Nikolaidis PT, Kontogiannis S, Trakada G. High-flow oxygen through nasal cannula vs. non-invasive ventilation in hypercapnic respiratory failure: a randomized clinical trial. Int J Environ Res Public Health 2020;17:5994. ArticlePubMedPMC
- 15. Lee MK, Choi J, Park B, Kim B, Lee SJ, Kim SH, et al. High flow nasal cannulae oxygen therapy in acute-moderate hypercapnic respiratory failure. Clin Respir J 2018;12:2046-56.ArticlePubMed
- 16. Huang Y, Lei W, Zhang W, Huang JA. High-flow nasal cannula in hypercapnic respiratory failure: a systematic review and meta-analysis. Can Respir J 2020;2020:7406457. ArticlePubMedPMC
References
Figure & Data
References
Citations
- Oxygénothérapie nasale à haut débit et insuffisance respiratoire aiguë hypercapnique
C. Girault, E. Artaud-Macari, G. Jolly, D. Carpentier, A. Cuvelier, G. Béduneau
Revue des Maladies Respiratoires.2024;[Epub] CrossRef - Safety and efficacy of high flow nasal canula in patients with mild hypercapnia
Mohammed A. Ibrahim, Magdy Emara, Mohammed Shehta
The Egyptian Journal of Bronchology.2023;[Epub] CrossRef - Current status of treatment of acute respiratory failure in Korea
Yong Jun Choi, Jae Hwa Cho
Journal of the Korean Medical Association.2022; 65(3): 124. CrossRef - High-flow nasal cannula: Evaluation of the perceptions of various performance aspects among Chinese clinical staff and establishment of a multidimensional clinical evaluation system
Ruoxuan Wen, Xingshuo Hu, Tengchen Wei, Kaifei Wang, Zhimei Duan, Zhanqi Zhao, Lixin Xie, Fei Xie
Frontiers in Medicine.2022;[Epub] CrossRef - The Application Progress of HFNC in Respiratory Diseases
迪 吴
Advances in Clinical Medicine.2022; 12(11): 10617. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-
- Related articles
-
- Combining reservoir mask oxygenation with high-flow nasal cannula in the treatment of hypoxemic respiratory failure among patients with COVID-19 pneumonia: a retrospective cohort study
- Percent fluid overload for prediction of fluid de-escalation in critically ill patients in Saudi Arabia: a prospective observational study

