Articles
- Page Path
- HOME > Acute Crit Care > Volume 38(2); 2023 > Article
-
Original Article
CPR/Resuscitation Prognostic significance of respiratory quotient in patients undergoing extracorporeal cardiopulmonary resuscitation in Korea -
Yun Im Lee1
 , Ryoung-Eun Ko2, Soo Jin Na2, Jeong-Am Ryu2,3, Yang Hyun Cho4, Jeong Hoon Yang2,5, Chi Ryang Chung2, Gee Young Suh2,6
, Ryoung-Eun Ko2, Soo Jin Na2, Jeong-Am Ryu2,3, Yang Hyun Cho4, Jeong Hoon Yang2,5, Chi Ryang Chung2, Gee Young Suh2,6 -
Acute and Critical Care 2023;38(2):190-199.
DOI: https://doi.org/10.4266/acc.2022.01438
Published online: May 25, 2023
1Department of Medicine, Dankook University Hospital, Dankook University School of Medicine, Cheonan, Korea
2Department of Critical Care Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
3Department of Neurosurgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
4Department of Thoracic and Cardiovascular Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
5Division of Cardiology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
6Division of Pulmonary and Critical Care Medicine, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- Corresponding author: Gee Young Suh Department of Critical Care Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 06351, Korea Tel: +82-2-3410-6399, Fax: +82-2-2148-7088, Email: suhgy@skku.edu
- *These authors contributed equally to this work.
Copyright © 2023 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background
- Respiratory quotient (RQ) may be used as a tissue hypoxia marker in various clinical settings but its prognostic significance in patients undergoing extracorporeal cardiopulmonary resuscitation (ECPR) is not known.
-
Methods
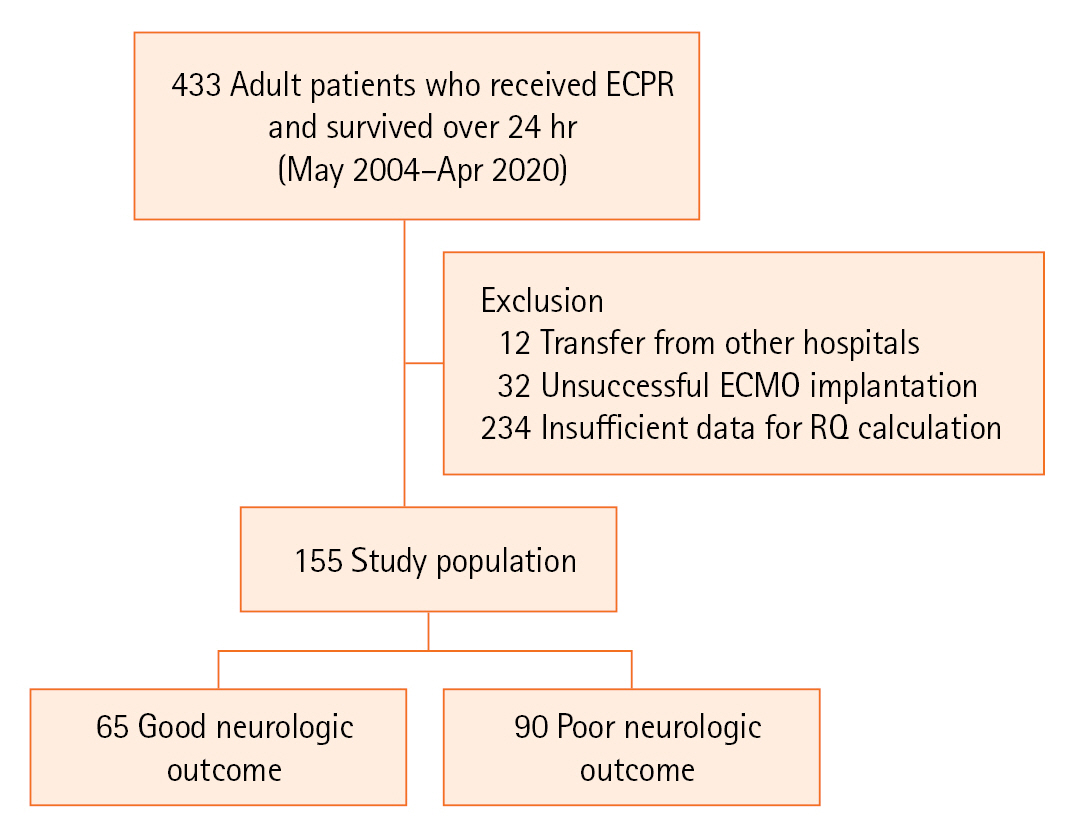
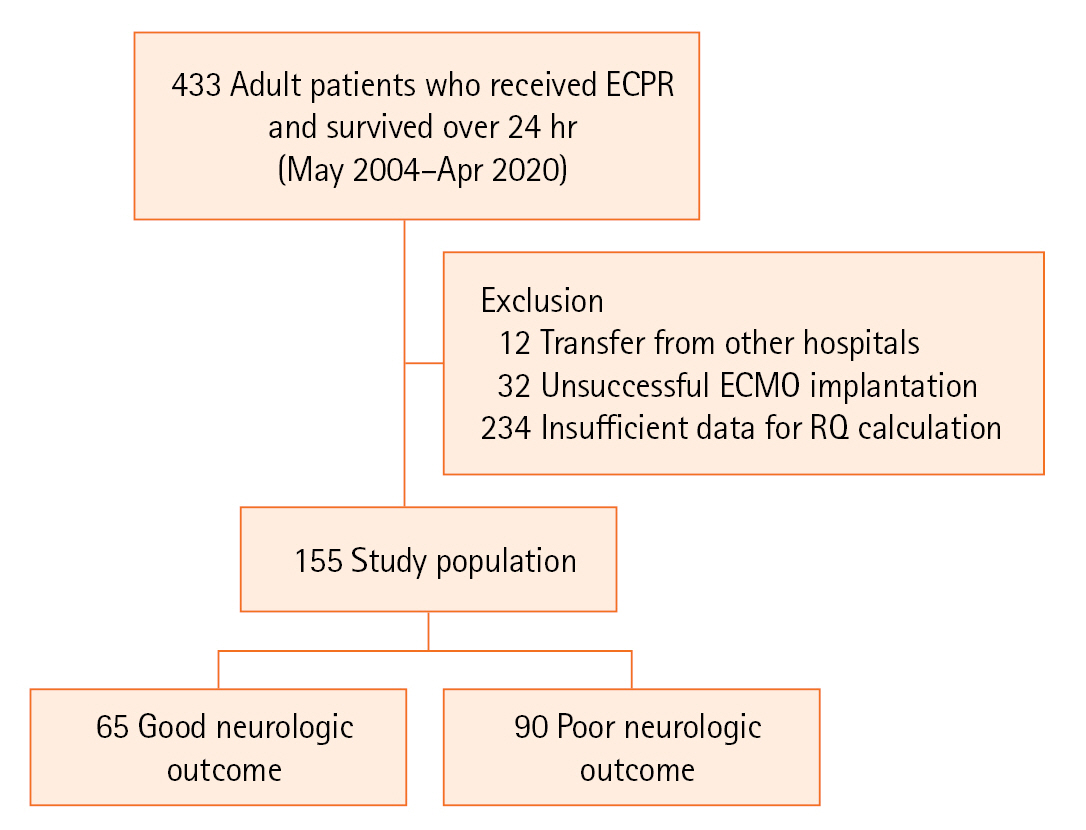
- Medical records of adult patients admitted to the intensive care units after ECPR in whom RQ could be calculated from May 2004 to April 2020 were retrospectively reviewed. Patients were divided into good neurologic outcome and poor neurologic outcome groups. Prognostic significance of RQ was compared to other clinical characteristics and markers of tissue hypoxia.
-
Results
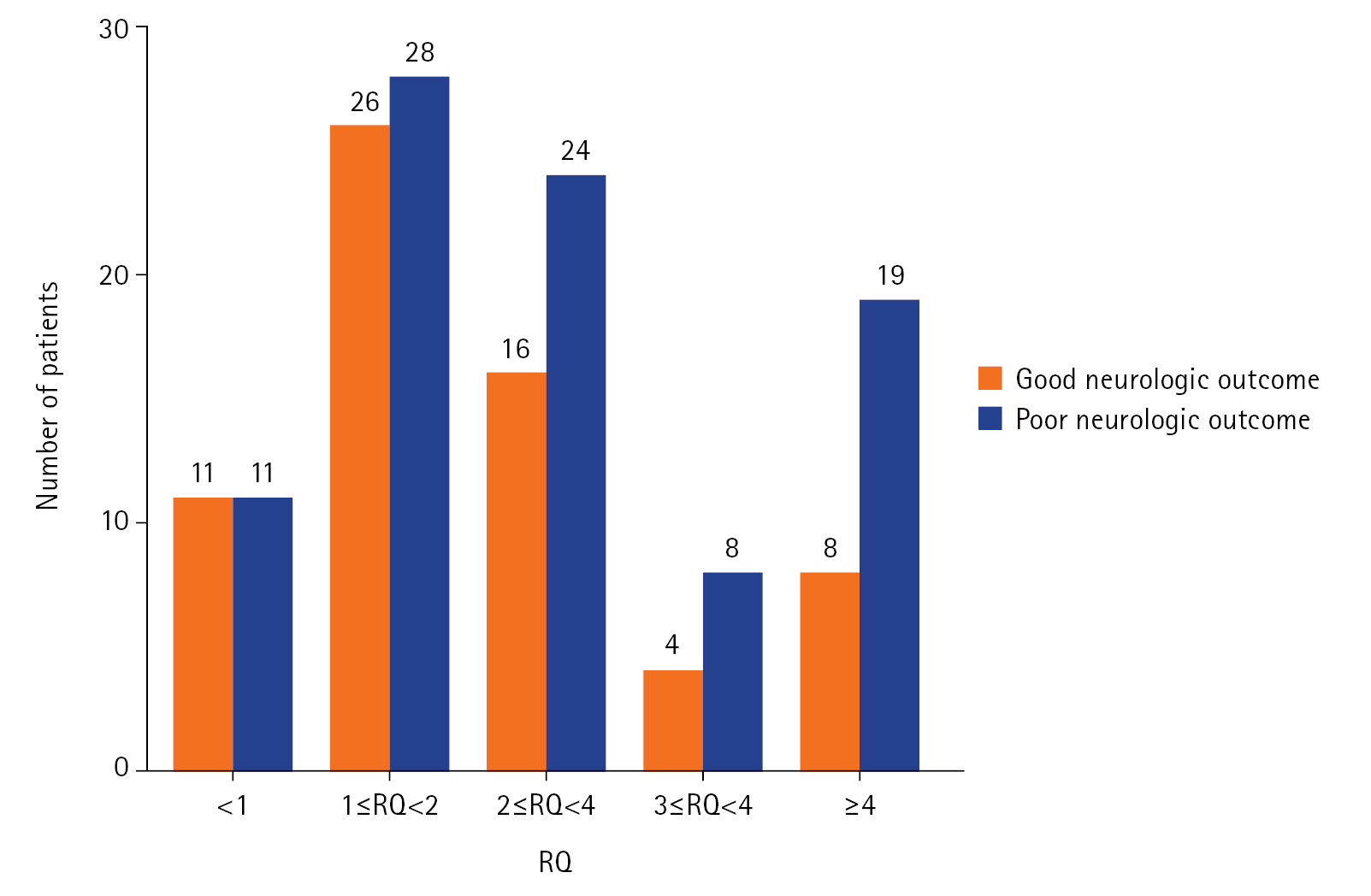
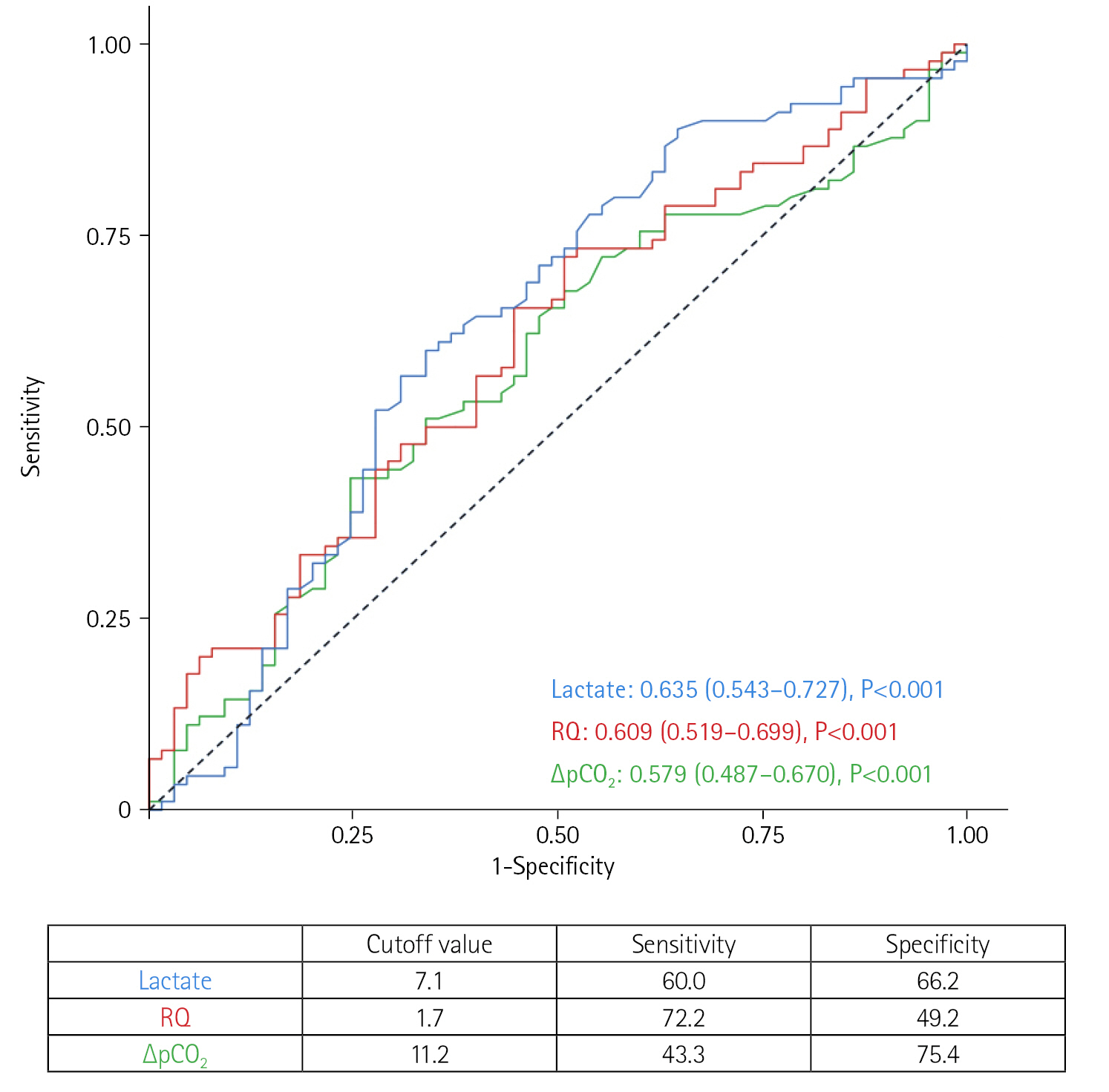
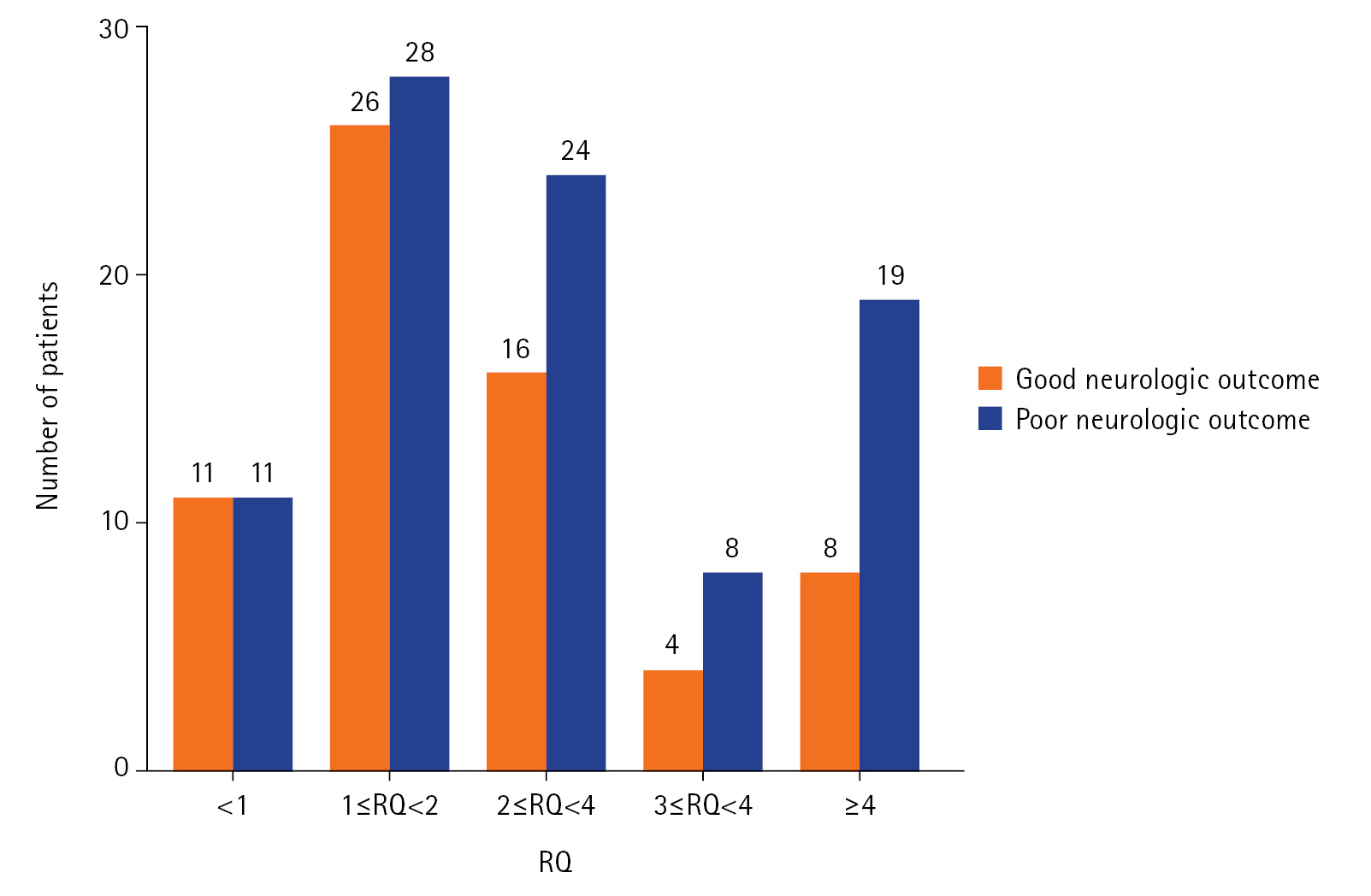
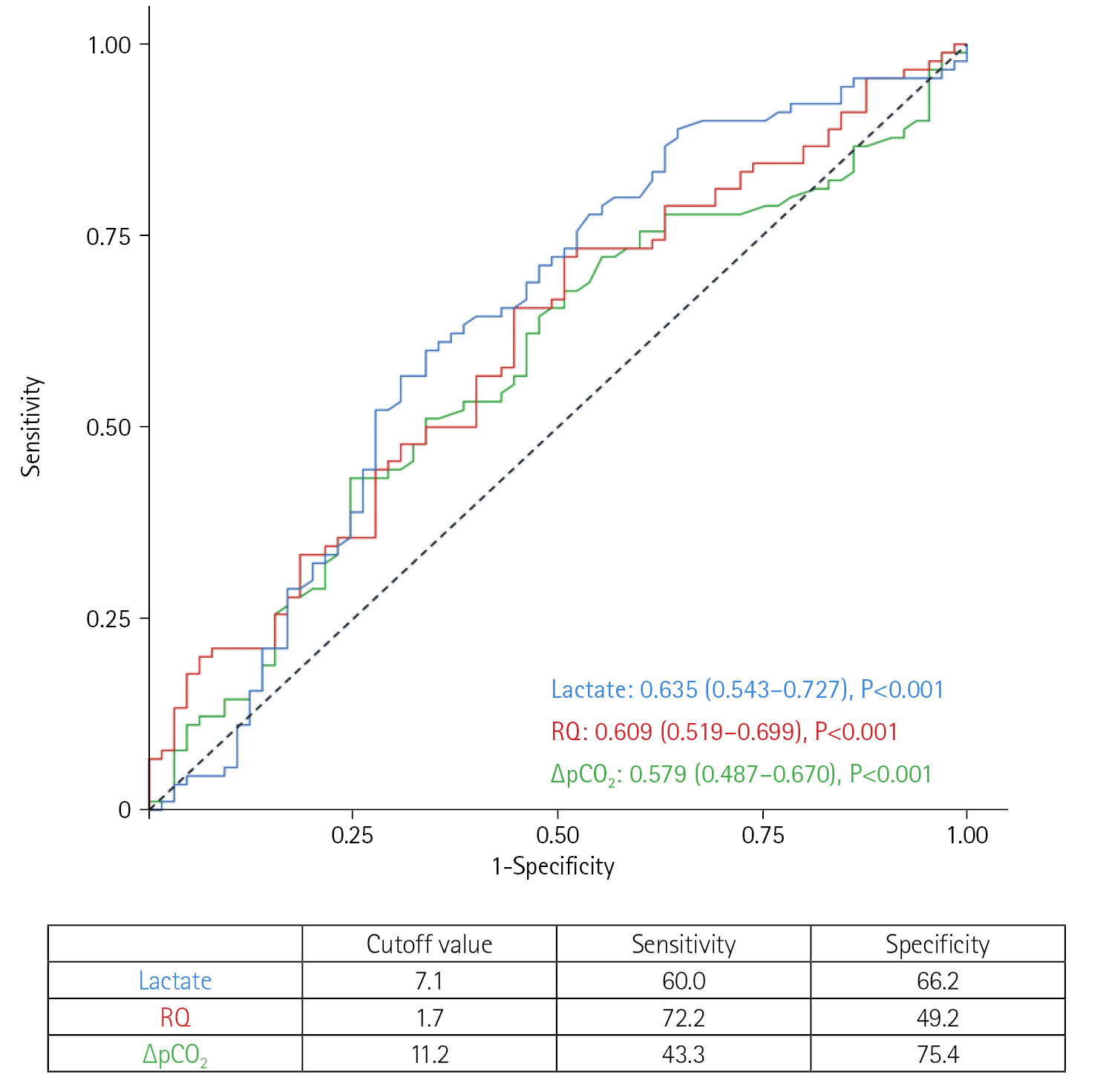
- During the study period, 155 patients were eligible for analysis. Of them, 90 (58.1%) had a poor neurologic outcome. The group with poor neurologic outcome had a higher incidence of out-of-hospital cardiac arrest (25.6% vs. 9.2%, P=0.010) and longer cardiopulmonary resuscitation to pump-on time (33.0 vs. 25.2 minutes, P=0.001) than the group with good neurologic outcome. For tissue hypoxia markers, the group with poor neurologic outcome had higher RQ (2.2 vs. 1.7, P=0.021) and lactate levels (8.2 vs. 5.4 mmol/L, P=0.004) than the group with good neurologic outcome. On multivariable analysis, age, cardiopulmonary resuscitation to pump-on time, and lactate levels above 7.1 mmol/L were significant predictors for a poor neurologic outcome but not RQ.
-
Conclusions
- In patients who received ECPR, RQ was not independently associated with poor neurologic outcome.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
DISCUSSION
KEY MESSAGES
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
FUNDING
This work was supported by the Korea Medical Device Development Fund grant funded by the Korea government (the Ministry of Science and ICT, the Ministry of Trade, Industry and Energy, the Ministry of Health & Welfare, the Ministry of Food and Drug Safety) (project no. 1711138313, KMDF_PR_20200901_0159).
-
AUTHOR CONTRIBUTIONS
Conceptualization: YIL, JHY, GYS. Data curation: YIL, REK. Formal analysis: YIL, REK, GYS. Funding acquisition: GYS. Methodology: JHY, CRC, GYS. Project administration: JHY, CRC, GYS. Visualization: YIL, REK. Writing–original draft: YIL, REK, GYS. Writing–review & editing: SJN, JAR, YHC.
NOTES
Acknowledgments
| Variable | Good neurologic outcome (n=65) | Poor neurologic outcome (n=90) | P-value |
|---|---|---|---|
| Age (yr) | 57 (47–65) | 67 (52–75) | 0.001 |
| Male | 50 (76.9) | 62 (68.9) | 0.270 |
| Body mass index (kg/m2) | 24.0 (21.3–27.2) | 24.0 (21.5–26.9) | 0.745 |
| Current smoker | 19 (29.2) | 17 (18.9) | 0.142 |
| Comorbidity (%) | |||
| Diabetes mellitus | 19 (29.2) | 35 (38.9) | 0.213 |
| Hypertension | 22 (33.8) | 49 (54.4) | 0.011 |
| Malignancy | 8 (12.3) | 11 (12.4) | 0.992 |
| Coronary artery disease | 10 (15.4) | 27 (30.0) | 0.035 |
| Peripheral arterial occlusive disease | 2 (3.1) | 6 (6.7) | 0.469 |
| Stroke | 4 (6.2) | 7 (7.9) | 0.761 |
| History of percutaneous coronary intervention | 14 (21.5) | 19 (21.3) | 0.977 |
| History of coronary artery bypass graft | 2 (3.1) | 9 (10.0) | 0.121 |
| Characteristics of ECPR | |||
| Location of ECMO implantation | 0.730 | ||
| Intensive care unit | 20 (30.8) | 36 (40.0) | |
| Catheterization laboratory | 27 (41.5) | 17 (18.9) | |
| Emergency room | 17 (26.2) | 35 (38.9) | |
| Operation room | 1 (1.5) | 2 (2.2) | |
| Out-of-hospital cardiac arrest | 6 (9.2) | 23 (25.6) | 0.010 |
| Initial shockable rhythm | 26 (40.0) | 32 (35.6) | 0.573 |
| Defibrillation | 34 (52.3) | 56 (62.2) | 0.217 |
| ROSC before ECMO implantation | 30 (46.9) | 35 (38.9) | 0.323 |
| CPR to pump-on time (min) | 25.2 (15.0–36.8) | 33.0 (24.0–47.0) | 0.001 |
| Initial SOFA scorea) | 14.0 (11.5–16.0) | 15.0 (13.0–17.0) | 0.005 |
Values are presented as median (interquartile range) or number (%).
ECPR: extracorporeal cardiopulmonary resuscitation; ECMO: extracorporeal membrane oxygenation; ROSC: return of spontaneous circulation; CPR: cardiopulmonary resuscitation; SOFA: Sequential Organ Failure Assessment.
a) SOFA score was calculated using worst values within 24 hours from ECPR. Cardiovascular variable was calculated as 4 in all cases.
- 1. Extracorporeal Life Support Organization (ELSO). ECLS international summary of statistics [Internet]. ELSO. 2022;[cited 2023 Apr 1]. Available from: https://www.elso.org/registry/internationalsummaryandreports/internationalsummary.aspx 2022.
- 2. Neumar RW, Shuster M, Callaway CW, Gent LM, Atkins DL, Bhanji F, et al. Part 1: executive summary. 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015;132(18 Suppl 2):S315-67.PubMed
- 3. Ko RE, Ryu JA, Cho YH, Sung K, Jeon K, Suh GY, et al. The differential neurologic prognosis of low-flow time according to the initial rhythm in patients who undergo extracorporeal cardiopulmonary resuscitation. Resuscitation 2020;148:121-7.ArticlePubMed
- 4. Belohlavek J, Smalcova J, Rob D, Franek O, Smid O, Pokorna M, et al. Effect of intra-arrest transport, extracorporeal cardiopulmonary resuscitation, and immediate invasive assessment and treatment on functional neurologic outcome in refractory out-of-hospital cardiac arrest: a randomized clinical trial. JAMA 2022;327:737-47.PubMedPMC
- 5. Bertic M, Worme M, Foroutan F, Rao V, Ross H, Billia F, et al. Predictors of survival and favorable neurologic outcome in patients treated with eCPR: a systematic review and meta-analysis. J Cardiovasc Transl Res 2022;15:279-90.ArticlePubMedPDF
- 6. Kliegel A, Losert H, Sterz F, Holzer M, Zeiner A, Havel C, et al. Serial lactate determinations for prediction of outcome after cardiac arrest. Medicine (Baltimore) 2004;83:274-9.ArticlePubMed
- 7. Garcia-Alvarez M, Marik P, Bellomo R. Sepsis-associated hyperlactatemia. Crit Care 2014;18:503. ArticlePubMedPMCPDF
- 8. Bakker J, Vincent JL, Gris P, Leon M, Coffernils M, Kahn RJ. Veno-arterial carbon dioxide gradient in human septic shock. Chest 1992;101:509-15.ArticlePubMed
- 9. Mecher CE, Rackow EC, Astiz ME, Weil MH. Venous hypercarbia associated with severe sepsis and systemic hypoperfusion. Crit Care Med 1990;18:585-9.ArticlePubMed
- 10. Mesquida J, Saludes P, Gruartmoner G, Espinal C, Torrents E, Baigorri F, et al. Central venous-to-arterial carbon dioxide difference combined with arterial-to-venous oxygen content difference is associated with lactate evolution in the hemodynamic resuscitation process in early septic shock. Crit Care 2015;19:126. ArticlePubMedPMCPDF
- 11. Mallat J, Lemyze M, Meddour M, Pepy F, Gasan G, Barrailler S, et al. Ratios of central venous-to-arterial carbon dioxide content or tension to arteriovenous oxygen content are better markers of global anaerobic metabolism than lactate in septic shock patients. Ann Intensive Care 2016;6:10. ArticlePubMedPMCPDF
- 12. Shinozaki K, Becker LB, Saeki K, Kim J, Yin T, Da T, et al. Dissociated oxygen consumption and carbon dioxide production in the post-cardiac arrest rat: a novel metabolic phenotype. J Am Heart Assoc 2018;7:e007721.ArticlePubMedPMC
- 13. Holzinger U, Brunner R, Losert H, Fuhrmann V, Herkner H, Madl C, et al. Resting energy expenditure and substrate oxidation rates correlate to temperature and outcome after cardiac arrest: a prospective observational cohort study. Crit Care 2015;19:128. ArticlePubMedPMCPDF
- 14. Park SB, Yang JH, Park TK, Cho YH, Sung K, Chung CR, et al. Developing a risk prediction model for survival to discharge in cardiac arrest patients who undergo extracorporeal membrane oxygenation. Int J Cardiol 2014;177:1031-5.ArticlePubMed
- 15. Lee JH, Ko RE, Park TK, Cho YH, Suh GY, Yang JH. Association between a multidisciplinary team approach and clinical outcomes in patients undergoing extracorporeal cardiopulmonary resuscitation in the emergency department. Korean Circ J 2021;51:908-18.ArticlePubMedPMCPDF
- 16. Ryu JA, Chung CR, Cho YH, Sung K, Suh GY, Park TK, et al. The association of findings on brain computed tomography with neurologic outcomes following extracorporeal cardiopulmonary resuscitation. Crit Care 2017;21:15. ArticlePubMedPMCPDF
- 17. Mekontso-Dessap A, Castelain V, Anguel N, Bahloul M, Schauvliege F, Richard C, et al. Combination of venoarterial PCO2 difference with arteriovenous O2 content difference to detect anaerobic metabolism in patients. Intensive Care Med 2002;28:272-7.ArticlePubMedPDF
- 18. Cummins RO, Chamberlain DA, Abramson NS, Allen M, Baskett PJ, Becker L, et al. Recommended guidelines for uniform reporting of data from out-of-hospital cardiac arrest: the Utstein Style. A statement for health professionals from a task force of the American Heart Association, the European Resuscitation Council, the Heart and Stroke Foundation of Canada, and the Australian Resuscitation Council. Circulation 1991;84:960-75.ArticlePubMed
- 19. Geocadin RG, Callaway CW, Fink EL, Golan E, Greer DM, Ko NU, et al. Standards for studies of neurological prognostication in comatose survivors of cardiac arrest: a scientific statement from the American Heart Association. Circulation 2019;140:e517-42.ArticlePubMed
- 20. Ospina-Tascón GA, Umaña M, Bermúdez W, Bautista-Rincón DF, Hernandez G, Bruhn A, et al. Combination of arterial lactate levels and venous-arterial CO2 to arterial-venous O2 content difference ratio as markers of resuscitation in patients with septic shock. Intensive Care Med 2015;41:796-805.ArticlePubMedPMCPDF
- 21. Gao X, Cao W, Li P. Pcv-aCO2/Ca-cvO2 combined with arterial lactate clearance rate as early resuscitation goals in septic shock. Am J Med Sci 2019;358:182-90.ArticlePubMed
- 22. Mesquida J, Espinal C, Saludes P, Cortés E, Pérez-Madrigal A, Gruartmoner G. Central venous-to-arterial carbon dioxide difference combined with arterial-to-venous oxygen content difference (PcvaCO2/CavO2) reflects microcirculatory oxygenation alterations in early septic shock. J Crit Care 2019;53:162-68.ArticlePubMed
- 23. Uber A, Grossestreuer AV, Ross CE, Patel PV, Trehan A, Donnino MW, et al. Preliminary observations in systemic oxygen consumption during targeted temperature management after cardiac arrest. Resuscitation 2018;127:89-94.ArticlePubMedPMC
- 24. Oshima T, Furukawa Y, Kobayashi M, Sato Y, Nihei A, Oda S. Fulfilling caloric demands according to indirect calorimetry may be beneficial for post cardiac arrest patients under therapeutic hypothermia. Resuscitation 2015;88:81-5.ArticlePubMed
- 25. Lee DH, Cho IS, Lee SH, Min YI, Min JH, Kim SH, et al. Correlation between initial serum levels of lactate after return of spontaneous circulation and survival and neurological outcomes in patients who undergo therapeutic hypothermia after cardiac arrest. Resuscitation 2015;88:143-9.ArticlePubMed
- 26. Riveiro DF, Oliveira VM, Braunner JS, Vieira SR. Evaluation of serum lactate, central venous saturation, and venous-arterial carbon dioxide difference in the prediction of mortality in postcardiac arrest syndrome. J Intensive Care Med 2016;31:544-52.ArticlePubMedPDF
- 27. Weil MH, Ruiz CE, Michaels S, Rackow EC. Acid-base determinants of survival after cardiopulmonary resuscitation. Crit Care Med 1985;13:888-92.ArticlePubMed
- 28. Choi KH, Yang JH, Park TK, Lee JM, Song YB, Hahn JY, et al. Risk prediction model of in-hospital mortality in patients with myocardial infarction treated with venoarterial extracorporeal membrane oxygenation. Rev Esp Cardiol (Engl Ed) 2019;72:724-31.ArticlePubMed
- 29. Kraut JA, Madias NE. Lactic acidosis. N Engl J Med 2014;371:2309-19.ArticlePubMed
- 30. Cipriani E, Langer T, Bottino N, Brusatori S, Carlesso E, Colombo SM, et al. Key role of respiratory quotient to reduce the occurrence of hypoxemia during extracorporeal gas exchange: a theoretical analysis. Crit Care Med 2020;48:e1327-31.ArticlePubMed
- 31. Su L, Tang B, Liu Y, Zhou G, Guo Q, He W, et al. P(v-a)CO2/C(a-v)O2-directed resuscitation does not improve prognosis compared with SvO2 in severe sepsis and septic shock: a prospective multicenter randomized controlled clinical study. J Crit Care 2018;48:314-20.ArticlePubMed
- 32. Monnet X, Julien F, Ait-Hamou N, Lequoy M, Gosset C, Jozwiak M, et al. Lactate and venoarterial carbon dioxide difference/arterial-venous oxygen difference ratio, but not central venous oxygen saturation, predict increase in oxygen consumption in fluid responders. Crit Care Med 2013;41:1412-20.ArticlePubMed
- 33. Li X, Yu X, Cheypesh A, Li J. Non-invasive measurements of energy expenditure and respiratory quotient by respiratory mass spectrometry in children on extracorporeal membrane oxygenation: a pilot study. Artif Organs 2015;39:815-9.ArticlePubMed
References
Figure & Data
References
Citations
- Risk factors for neurological disability outcomes in patients under extracorporeal membrane oxygenation following cardiac arrest: An observational study
Amir Vahedian-Azimi, Ibrahim Fawzy Hassan, Farshid Rahimi-Bashar, Hussam Elmelliti, Anzila Akbar, Ahmed Labib Shehata, Abdulsalam Saif Ibrahim, Ali Ait Hssain
Intensive and Critical Care Nursing.2024; 83: 103674. CrossRef - What factors are effective on the CPR duration of patients under extracorporeal cardiopulmonary resuscitation: a single-center retrospective study
Amir Vahedian-Azimi, Ibrahim Fawzy Hassan, Farshid Rahimi-Bashar, Hussam Elmelliti, Anzila Akbar, Ahmed Labib Shehata, Abdulsalam Saif Ibrahim, Ali Ait Hssain
International Journal of Emergency Medicine.2024;[Epub] CrossRef - Extracorporeal cardiopulmonary resuscitation for out-of-hospital cardiac arrest and in-hospital cardiac arrest with return of spontaneous circulation: be careful when comparing apples to oranges
Hwa Jin Cho, In Seok Jeong, Jan Bělohlávek
Acute and Critical Care.2023; 38(2): 242. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite