
Articles
- Page Path
- HOME > Acute Crit Care > Volume 31(2); 2016 > Article
- Case Report Extracorporeal Membrane Oxygenation Cannula Malposition in the Azygos Vein in a Neonate with Right-Sided Congenital Diaphragmatic Hernia
- Seung Jun Choi, M.D.1, Chun-Soo Park, M.D., Ph.D.2, Won Kyoung Jhang, M.D., Ph.D.1, Seong Jong Park, M.D., Ph.D.1
-
Korean Journal of Critical Care Medicine 2016;31(2):152-155.
DOI: https://doi.org/10.4266/kjccm.2016.31.2.152
Published online: May 31, 2016
1Division of Pediatric Critical Care Medicine, Asan Medical Center Children's Hospital, Seoul, Korea
2Division of Pediatric Cardiac Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- Correspondence to: Seong Jong Park, Division of Pediatric Critical Care Medicine, Department of Pediatrics, Asan Medical Center Children’s Hospital, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpa-gu, Seoul 05505, Korea Tel: +82-2-3010-3390, Fax: +82-2-3010-3725 E-mail: drpsj@amc.seoul.kr
• Received: January 20, 2016 • Revised: March 3, 2016 • Accepted: March 7, 2016
Copyright © 2016 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 8,072 Views
- 90 Download
- 4 Crossref
Abstract
- Malposition of the extracorporeal membrane oxygenation (ECMO) venous cannula in the azygos vein is not frequently reported. We hereby present such a case, which occurred in a neonate with right-sided congenital diaphragmatic hernia. Despite ECMO application, neither adequate flow nor sufficient oxygenation was achieved. On the cross-table lateral chest radiograph, the cannula tip was identified posterior to the heart silhouette, which implied malposition of the cannula in the azygos vein. After repositioning the cannula, the target flow and oxygenation were successfully achieved. When sufficient venous flow is not achieved, as in our case, clinicians should be alerted so they can identify the cannula tip location on lateral chest radiograph and confirm whether malposition in the azygos vein is the cause of the ineffective ECMO.
Case Report
Discussion
Fig. 1.Antero-posterior chest radiograph after admission. Typical findings of right-sided CDH is noticed – bowel gas is present on the right lung field, and the heart and mediastinum are deviated to the left. CDH: congenital diaphragmatic hernia.

Fig. 2.Antero-posterior chest radiograph after ECMO cannulation. Total lung haziness is noticed due to ARDS and combined heart failure, thereby obliterating the cardiac silhouette. ECMO: extracorporeal membrane oxygenation; ARDS: acute respiratory distress syndrome; VC: venous cannula; AC: arterial cannula.
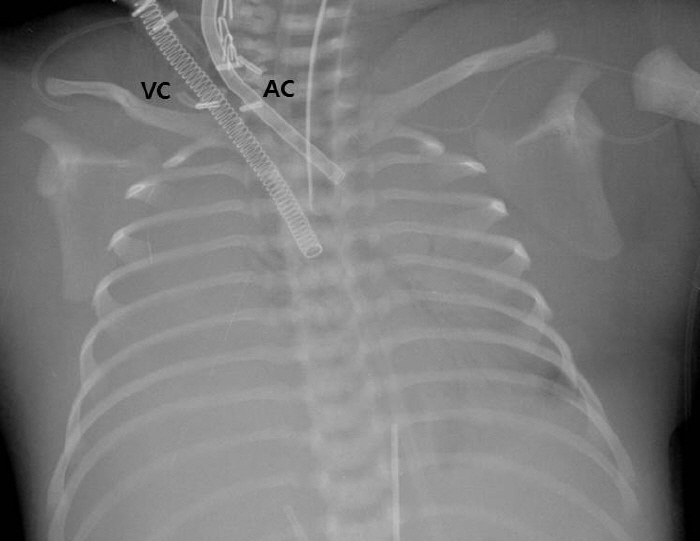
Fig. 3.Cross-table lateral chest radiographs showing the cannula tip positioned posterior to the cardiac silhouette (A), and anterior in the superior vena cava after adjustment (B).

- 1. Hedrick HL, Crombleholme TM, Flake AW, Nance ML, von Allmen D, Howell LJ, et al. Right congenital diaphragmatic hernia: prenatal assessment and outcome. J Pediatr Surg 2004;39:319-23.ArticlePubMed
- 2. Boloker J, Bateman DA, Wung JT, Stolar CJ. Congenital diaphragmatic hernia in 120 infants treated consecutively with permissive hypercapnea/spontaneous respiration/elective repair. J Pediatr Surg 2002;37:357-66.ArticlePubMed
- 3. Fisher JC, Jefferson RA, Kuenzler KA, Stolar CJ, Arkovitz MS. Challenges to cannulation for extracorporeal support in neonates with right-sided congenital diaphragmatic hernia. J Pediatr Surg 2007;42:2123-8.ArticlePubMed
- 4. Byrnes J, Prodhan P, Imamura M, Frazier E. Accidental azygos vein extracorporeal membrane oxygenation cannulation in a neonate with premature closure of the ductus arteriosus. ASAIO J 2011;57:344-5.ArticlePubMed
- 5. Balmaks R, Sufficool KE, White FV, Byrge MM, Kolovos NS. Extracorporeal membrane oxygenation cannula malposition in the azygos vein in an infant. Int J Artif Organs 2013;36:518-21.ArticlePubMed
- 6. Irish MS, O’Toole SJ, Kapur P, Bambini DA, Azizkhan RG, Allen JE, et al. Cervical ECMO cannula placement in infants and children: recommendations for assessment of adequate positioning and function. J Pediatr Surg 1998;33:929-31.ArticlePubMed
- 7. Thomas TH, Price R, Ramaciotti C, Thompson M, Megison S, Lemler MS. Echocardiography, not chest radiography, for evaluation of cannula placement during pediatric extracorporeal membrane oxygenation. Pediatr Crit Care Med 2009;10:56-9.ArticlePubMed
References
Figure & Data
References
Citations
Citations to this article as recorded by 
- Inadvertent cannulation of the azygos vein during eCPR
Shelina M. Jamal, Deborah S. Fruitman, Kevin M. Lichtenstein, Darren H. Freed, Natalie L. Yanchar
Journal of Pediatric Surgery Case Reports.2021; 71: 101941. CrossRef - Identification of Inadvertent Azygous Vein Cannulation Using Transthoracic Echocardiography During Venoarterial Extracorporeal Membrane Oxygenation Initiation
Bethany G. Runkel, Jason D. Fraser, John M. Daniel, Karina M. Carlson
CASE.2019; 3(2): 67. CrossRef - Successful Extracorporeal Membrane Oxygenation After Incidental Azygos Vein Cannulation in a Neonate With Right-Sided Congenital Diaphragmatic Hernia Interruption of the Inferior Vena Cava and Azygos Continuation
Alessandra Mayer, Genny Raffaeli, Federico Schena, Valeria Parente, Gabriele Sorrentino, Francesco Macchini, Anna Maria Colli, Lucia Mauri, Simona Neri, Irene Borzani, Ernesto Leva, Fabio Mosca, Giacomo Cavallaro
Frontiers in Pediatrics.2019;[Epub] CrossRef - The Future of Research on Extracorporeal Membrane Oxygenation (ECMO)
Ji Young Lee
Korean Journal of Critical Care Medicine.2016; 31(2): 73. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite



