
Articles
- Page Path
- HOME > Acute Crit Care > Volume 37(3); 2022 > Article
-
Original Article
Infection In-hospital mortality prediction using frailty scale and severity score in elderly patients with severe COVID-19 -
Yong Sub Na1
 , Jin Hyoung Kim2, Moon Seong Baek3, Won-Young Kim3, Ae-Rin Baek4, Bo young Lee5, Gil Myeong Seong6, Song-I Lee7
, Jin Hyoung Kim2, Moon Seong Baek3, Won-Young Kim3, Ae-Rin Baek4, Bo young Lee5, Gil Myeong Seong6, Song-I Lee7 -
Acute and Critical Care 2022;37(3):303-311.
DOI: https://doi.org/10.4266/acc.2022.00017
Published online: July 5, 2022
1Department of Pulmonology and Critical Care Medicine, Chosun University Hospital, Gwangju, Korea
2Division of Respiratory and Critical Care Medicine, Department of Internal Medicine, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea
3Department of Internal Medicine, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea
4Division of Allergy and Pulmonology, Department of Internal Medicine, Soonchunhyang University Bucheon Hospital, Bucheon, Korea
5Division of Allergy and Respiratory Diseases, Soonchunhyang University Hospital, Seoul, Korea
6Department of Internal Medicine, Jeju National University College of Medicine, Jeju, Korea
7Department of Pulmonary and Critical Care Medicine, Chungnam National University Hospital, Daejeon, Korea
- Corresponding author: Song-I Lee Department of Pulmonary and Critical Care Medicine, Chungnam National University Hospital, 282 Munhwa-ro, Jung-gu, Daejeon 35015, Korea Tel: +82-42-280-6816, Fax: +82-42-257-5753, E-mail: newcomet01@naver.com
- *These authors contributed equally to this study.
Copyright © 2022 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background
- Elderly patients with coronavirus disease 2019 (COVID-19) have a high disease severity and mortality. However, the use of the frailty scale and severity score to predict in-hospital mortality in the elderly is not well established. Therefore, in this study, we investigated the use of these scores in COVID-19 cases in the elderly.
-
Methods
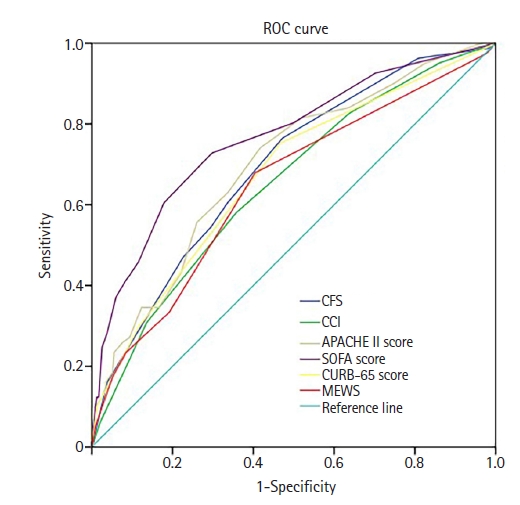
- This multicenter retrospective study included severe COVID-19 patients admitted to seven hospitals in Korea from February 2020 to February 2021. We evaluated patients’ Acute Physiology and Chronic Health Evaluation (APACHE) II score; confusion, urea nitrogen, respiratory rate, blood pressure, 65 years of age and older (CURB-65) score; modified early warning score (MEWS); Sequential Organ Failure Assessment (SOFA) score; clinical frailty scale (CFS) score; and Charlson comorbidity index (CCI). We evaluated the predictive value using receiver operating characteristic (ROC) curve analysis.
-
Results
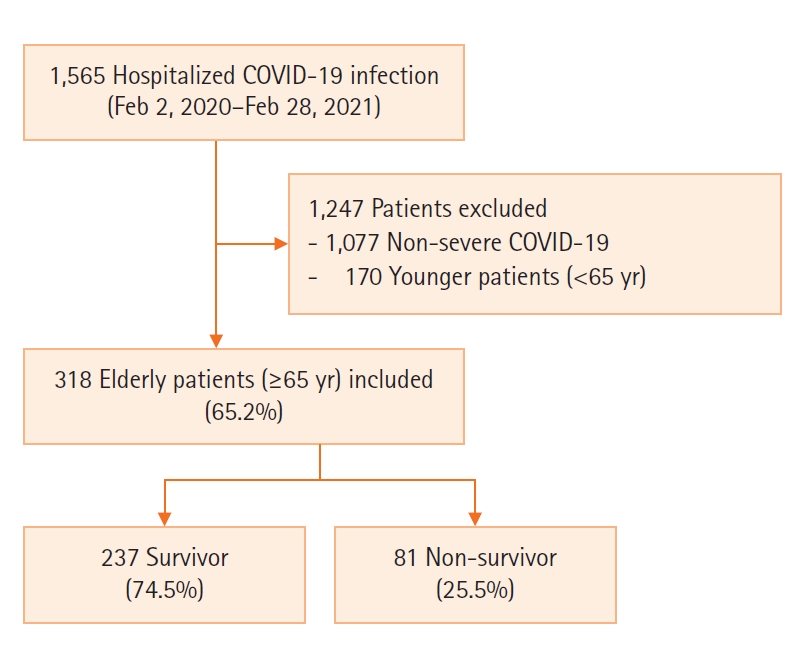
- The study included 318 elderly patients with severe COVID-19 of whom 237 (74.5%) were survivors and 81 (25.5%) were non-survivors. The non-survivor group was older and had more comorbidities than the survivor group. The CFS, CCI, APACHE II, SOFA, CURB-65, and MEWS scores were higher in the non-survivor group than in the survivor group. When analyzed using the ROC curve, SOFA score showed the best performance in predicting the prognosis of elderly patients (area under the curve=0.766, P<0.001). CFS and SOFA scores were associated with in-hospital mortality in the multivariate analysis.
-
Conclusions
- The SOFA score is an efficient tool for assessing in-hospital mortality in elderly patients with severe COVID-19.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
DISCUSSION
Key Message
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conceptualization: YSN, JHK, SIL. Data curation: all authors. Formal analysis: SIL. Methodology: SIL. Visualization: YSN, JHK, SIL. Writing–original draft: all authors. Writing–review & editing: all authors.
NOTES
Values are presented as median (interquartile range) or number (%).
COVID-19: coronavirus disease 2019; DM: diabetes mellitus; COPD: chronic obstructive pulmonary disease; SBP: systolic blood pressure; DBP: diastolic blood pressure; HR: heart rate; RR: respiratory rate; SpO2: saturation pulse oxygen; GCS: Glasgow coma scale; BUN: blood urea nitrogen.
Values are presented as median (interquartile range).
COVID-19: coronavirus disease 2019; APACHE: Acute Physiology and Chronic Health Evaluation, SOFA: Sequential Organ Failure Assessment, CURB-65: confusion, urea nitrogen, respiratory rate, blood pressure, 65 years of age and older, MEWS: Modified Early Warning.
OR: odds ratio; CI: confidence interval; APACHE: Acute Physiology and Chronic Health Evaluation; SOFA: Sequential Organ Failure Assessment; CURB-65: confusion, urea nitrogen, respiratory rate, blood pressure, 65 years of age and older; MEWS: modified early warning score; DM: diabetes mellitus; COPD: chronic obstructive pulmonary disease.
- 1. Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta Biomed 2020;91:157-60.PubMedPMC
- 2. Bajema KL, Dahl RM, Evener SL, Prill MM, Rodriguez-Barradas MC, Marconi VC. Comparative effectiveness and antibody responses to moderna and Pfizer-BioNTech COVID-19 vaccines among hospitalized veterans: five veterans affairs medical centers, United States, February 1-September 30, 2021. MMWR Morb Mortal Wkly Rep 2021;70:1700-5.ArticlePubMedPMC
- 3. Baden LR, El Sahly HM, Essink B, Kotloff K, Frey S, Novak R, et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N Engl J Med 2021;384:403-16.ArticlePubMedPMC
- 4. Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med 2020;383:2603-15.ArticlePubMedPMC
- 5. World Health Organization. COVID-19, Korea [Internet]. Geneva, World Health Organization. 2021;[cited 2021 Dec 20]. Available from: https://covid19.who.int/region/wpro/country/kr.
- 6. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020;395:497-506.ArticlePubMedPMC
- 7. Ruan Q, Yang K, Wang W, Jiang L, Song J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med 2020;46:846-8.ArticlePubMedPMCPDF
- 8. Zhang L, Hou J, Ma FZ, Li J, Xue S, Xu ZG. The common risk factors for progression and mortality in COVID-19 patients: a meta-analysis. Arch Virol 2021;166:2071-87.ArticlePubMedPMCPDF
- 9. Booth A, Reed AB, Ponzo S, Yassaee A, Aral M, Plans D, et al. Population risk factors for severe disease and mortality in COVID-19: a global systematic review and meta-analysis. PLoS One 2021;16:e0247461.ArticlePubMedPMC
- 10. Guo T, Shen Q, Guo W, He W, Li J, Zhang Y, et al. Clinical characteristics of elderly patients with COVID-19 in Hunan Province, China: a multicenter, retrospective study. Gerontology 2020;66:467-75.ArticlePubMedPDF
- 11. Singhal S, Kumar P, Singh S, Saha S, Dey AB. Clinical features and outcomes of COVID-19 in older adults: a systematic review and meta-analysis. BMC Geriatr 2021;21:321. ArticlePubMedPMCPDF
- 12. Liu K, Chen Y, Lin R, Han K. Clinical features of COVID-19 in elderly patients: a comparison with young and middle-aged patients. J Infect 2020;80:e14-e18.ArticlePubMedPMC
- 13. Pepe M, Maroun-Eid C, Romero R, Arroyo-Espliguero R, Fernàndez-Rozas I, Aparisi A, et al. Clinical presentation, therapeutic approach, and outcome of young patients admitted for COVID-19, with respect to the elderly counterpart. Clin Exp Med 2021;21:249-68.ArticlePubMedPMCPDF
- 14. Owen RK, Conroy SP, Taub N, Jones W, Bryden D, Pareek M, et al. Comparing associations between frailty and mortality in hospitalised older adults with or without COVID-19 infection: a retrospective observational study using electronic health records. Age Ageing 2021;50:307-16.ArticlePubMedPMCPDF
- 15. Aw D, Woodrow L, Ogliari G, Harwood R. Association of frailty with mortality in older inpatients with Covid-19: a cohort study. Age Ageing 2020;49:915-22.ArticlePubMedPMCPDF
- 16. Pranata R, Henrina J, Lim MA, Lawrensia S, Yonas E, Vania R, et al. Clinical frailty scale and mortality in COVID-19: a systematic review and dose-response meta-analysis. Arch Gerontol Geriatr 2021;93:104324. ArticlePubMedPMC
- 17. Raith EP, Udy AA, Bailey M, McGloughlin S, MacIsaac C, Bellomo R, et al. Prognostic accuracy of the SOFA score, SIRS criteria, and qSOFA score for in-hospital mortality among adults with suspected infection admitted to the intensive care unit. JAMA 2017;317:290-300.ArticlePubMed
- 18. Yang Z, Hu Q, Huang F, Xiong S, Sun Y. The prognostic value of the SOFA score in patients with COVID-19: a retrospective, observational study. Medicine (Baltimore) 2021;100:e26900.ArticlePubMedPMC
- 19. Pulok MH, Theou O, van der Valk AM, Rockwood K. The role of illness acuity on the association between frailty and mortality in emergency department patients referred to internal medicine. Age Ageing 2020;49:1071-9.ArticlePubMedPMCPDF
- 20. Gandhi RT, Lynch JB, Del Rio C. Mild or moderate Covid-19. N Engl J Med 2020;383:1757-66.ArticlePubMed
- 21. Vrillon A, Hourregue C, Azuar J, Grosset L, Boutelier A, Tan S, et al. COVID-19 in older adults: a series of 76 patients aged 85 years and older with COVID-19. J Am Geriatr Soc 2020;68:2735-43.ArticlePubMedPMCPDF
- 22. Herrmann ML, Hahn JM, Walter-Frank B, Bollinger DM, Schmauder K, Schnauder G, et al. COVID-19 in persons aged 70+ in an early affected German district: Risk factors, mortality and post-COVID care needs: a retrospective observational study of hospitalized and non-hospitalized patients. PLoS One 2021;16:e0253154.ArticlePubMedPMC
- 23. Knopp P, Miles A, Webb TE, Mcloughlin BC, Mannan I, Raja N, et al. Presenting features of COVID-19 in older people: relationships with frailty, inflammation and mortality. Eur Geriatr Med 2020;11:1089-94.ArticlePubMedPMCPDF
- 24. Lee JY, Kim HA, Huh K, Hyun M, Rhee JY, Jang S, et al. Risk factors for mortality and respiratory support in elderly patients hospitalized with COVID-19 in Korea. J Korean Med Sci 2020;35:e223.ArticlePubMedPMCPDF
- 25. Leung C. Risk factors for predicting mortality in elderly patients with COVID-19: a review of clinical data in China. Mech Ageing Dev 2020;188:111255. ArticlePubMedPMC
- 26. Gao S, Jiang F, Jin W, Shi Y, Yang L, Xia Y, et al. Risk factors influencing the prognosis of elderly patients infected with COVID-19: a clinical retrospective study in Wuhan, China. Aging (Albany NY) 2020;12:12504-16.ArticlePubMedPMC
- 27. Li P, Chen L, Liu Z, Pan J, Zhou D, Wang H, et al. Clinical features and short-term outcomes of elderly patients with COVID-19. Int J Infect Dis 2020;97:245-50.ArticlePubMedPMC
- 28. Tuty Kuswardhani RA, Henrina J, Pranata R, Anthonius Lim M, Lawrensia S, Suastika K. Charlson comorbidity index and a composite of poor outcomes in COVID-19 patients: a systematic review and meta-analysis. Diabetes Metab Syndr 2020;14:2103-9.ArticlePubMedPMC
- 29. Joynt GM, Leung AK, Ho CM, So D, Shum HP, Chow FL, et al. Admission triage tool for adult intensive care unit admission in Hong Kong during the COVID-19 outbreak. Hong Kong Med J 2022;28:64-72.ArticlePubMed
- 30. Sprung CL, Joynt GM, Christian MD, Truog RD, Rello J, Nates JL. Adult ICU triage during the coronavirus disease 2019 pandemic: who will live and who will die? Recommendations to improve survival. Crit Care Med 2020;48:1196-202.ArticlePubMedPMC
- 31. Aziz S, Arabi YM, Alhazzani W, Evans L, Citerio G, Fischkoff K, et al. Managing ICU surge during the COVID-19 crisis: rapid guidelines. Intensive Care Med 2020;46:1303-25.ArticlePubMedPMCPDF
- 32. Jung C, Flaatten H, Fjølner J, Bruno RR, Wernly B, Artigas A, et al. The impact of frailty on survival in elderly intensive care patients with COVID-19: the COVIP study. Crit Care 2021;25:149. ArticlePubMedPMC
- 33. Aliberti MJ, Szlejf C, Avelino-Silva VI, Suemoto CK, Apolinario D, Dias MB, et al. COVID-19 is not over and age is not enough: using frailty for prognostication in hospitalized patients. J Am Geriatr Soc 2021;69:1116-27.ArticlePubMedPMCPDF
- 34. Berenguer J, Borobia AM, Ryan P, Rodríguez-Baño J, Bellón JM, Jarrín I, et al. Development and validation of a prediction model for 30-day mortality in hospitalised patients with COVID-19: the COVID-19 SEIMC score. Thorax 2021;76:920-9.ArticlePubMedPMC
- 35. Alves VP, Casemiro FG, Araujo BG, Lima MA, Oliveira RS, Fernandes FT, et al. Factors associated with mortality among elderly people in the COVID-19 pandemic (SARS-CoV-2): a systematic review and meta-analysis. Int J Environ Res Public Health 2021;18:8008. ArticlePubMedPMC
- 36. Dessie ZG, Zewotir T. Mortality-related risk factors of COVID-19: a systematic review and meta-analysis of 42 studies and 423,117 patients. BMC Infect Dis 2021;21:855. ArticlePubMedPMCPDF
References
Figure & Data
References
Citations
- Risk factors for progressing to critical illness in patients with hospital-acquired COVID-19
Kyung-Eui Lee, Jinwoo Lee, Sang-Min Lee, Hong Yeul Lee
The Korean Journal of Internal Medicine.2024; 39(3): 477. CrossRef - Omicron, Long-COVID, and the Safety of Elective Surgery for Adults and Children: Joint Guidance from the Therapeutics and Guidelines Committee of the Surgical Infection Society and the Surgery Strategic Clinical Network, Alberta Health Services
Philip S. Barie, Mary E. Brindle, Rachel G. Khadaroo, Tara L. Klassen, Jared M. Huston
Surgical Infections.2023; 24(1): 6. CrossRef - Evaluation of risk scores as predictors of mortality and hospital length of stay for older COVID‐19 patients
Banu Buyukaydin, Tahsin Karaaslan, Omer Uysal
AGING MEDICINE.2023; 6(1): 56. CrossRef - Atypical presentation of COVID-19 in older patients is associated with frailty but not with adverse outcomes
Joy E. van Son, Elisabeth C. P. Kahn, Jessica M. van der Bol, Dennis G. Barten, Laura C. Blomaard, Carmen van Dam, Jacobien Ellerbroek, Steffy W. M. Jansen, Anita Lekx, Carolien M. J. van der Linden, Roy Looman, Huub A. A. M. Maas, Francesco U. S. Mattace
European Geriatric Medicine.2023;[Epub] CrossRef - Neurological Manifestations and Complications of the Central Nervous System as Risk Factors and Predictors of Mortality in Patients Hospitalized with COVID-19: A Cohort Study
Ana Luisa Corona-Nakamura, Martha Judith Arias-Merino, Rayo Morfín-Otero, Guillermo Rodriguez-Zavala, Alfredo León-Gil, Juan Ramsés Camarillo-Escalera, Idarmis Brisseida Reyes-Cortés, María Gisela Valdovinos-Ortega, Erick René Nava-Escobar, Ana María de l
Journal of Clinical Medicine.2023; 12(12): 4065. CrossRef - Modified Early Warning Score: Clinical Deterioration of Mexican Patients Hospitalized with COVID-19 and Chronic Disease
Nicolás Santiago González, María de Lourdes García-Hernández, Patricia Cruz-Bello, Lorena Chaparro-Díaz, María de Lourdes Rico-González, Yolanda Hernández-Ortega
Healthcare.2023; 11(19): 2654. CrossRef - Risk Factors and Predictive Model for Mortality of Hospitalized COVID-19 Elderly Patients from a Tertiary Care Hospital in Thailand
Mallika Chuansangeam, Bunyarat Srithan, Pattharawin Pattharanitima, Pawit Phadungsaksawasdi
Medicines.2023; 10(11): 59. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite


