
Articles
- Page Path
- HOME > Acute Crit Care > Volume 38(1); 2023 > Article
-
Original Article
Epidemiology Risk factors for hospital mortality in intensive care unit survivors: a retrospective cohort study -
Luiza Gabriella Antonio e Silva1
 , Claudia Maria Dantas de Maio Carrilho2, Thalita Bento Talizin3, Lucienne Tibery Queiroz Cardoso2, Edson Lopes Lavado4, Cintia Magalhães Carvalho Grion2
, Claudia Maria Dantas de Maio Carrilho2, Thalita Bento Talizin3, Lucienne Tibery Queiroz Cardoso2, Edson Lopes Lavado4, Cintia Magalhães Carvalho Grion2 -
Acute and Critical Care 2023;38(1):68-75.
DOI: https://doi.org/10.4266/acc.2022.01375
Published online: February 27, 2023
1Universidade Estadual de Londrina, Londrina, Brazil
2Departamento de Clínica Médica, Universidade Estadual de Londrina, Londrina, Brazil
3Departamento de Cirurgia Geral, Universidade de São Paulo, São Paulo, Brazil
4Departamento de Fisioterapia, Universidade Estadual de Londrina, São Paulo, Brazil
- Corresponding author: Cintia Magalhães Carvalho Grion Departamento de Clínica Médica, Universidade Estadual de Londrina,. Rua Robert Koch 60, Vila Operária. Londrina, Paraná 86038-440, Brasil Tel: +55-43-33712284 Fax: +55-43-33712466 Email: cintiagrion@hotmail.com
Copyright © 2023 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, providewere observed among non-survivors. In the logisticd the original work is properly cited.
Abstract
-
Background
- Deaths can occur after a patient has survived treatment for a serious illness in an intensive care unit (ICU). Mortality rates after leaving the ICU can be considered indicators of health care quality. This study aims to describe risk factors and mortality of surviving patients discharged from an ICU in a university hospital.
-
Methods
- Retrospective cohort study carried out from January 2017 to December 2018. Data on age, sex, length of hospital stay, diagnosis on admission to the ICU, hospital discharge outcome, presence of infection, and Simplified Acute Physiology Score (SAPS) III prognostic score were collected. Infected patients were considered as those being treated for an infection on discharge from the ICU. Patients were divided into survivors and non-survivors on leaving the hospital. The association between the studied variables was performed using the logistic regression model.
-
Results
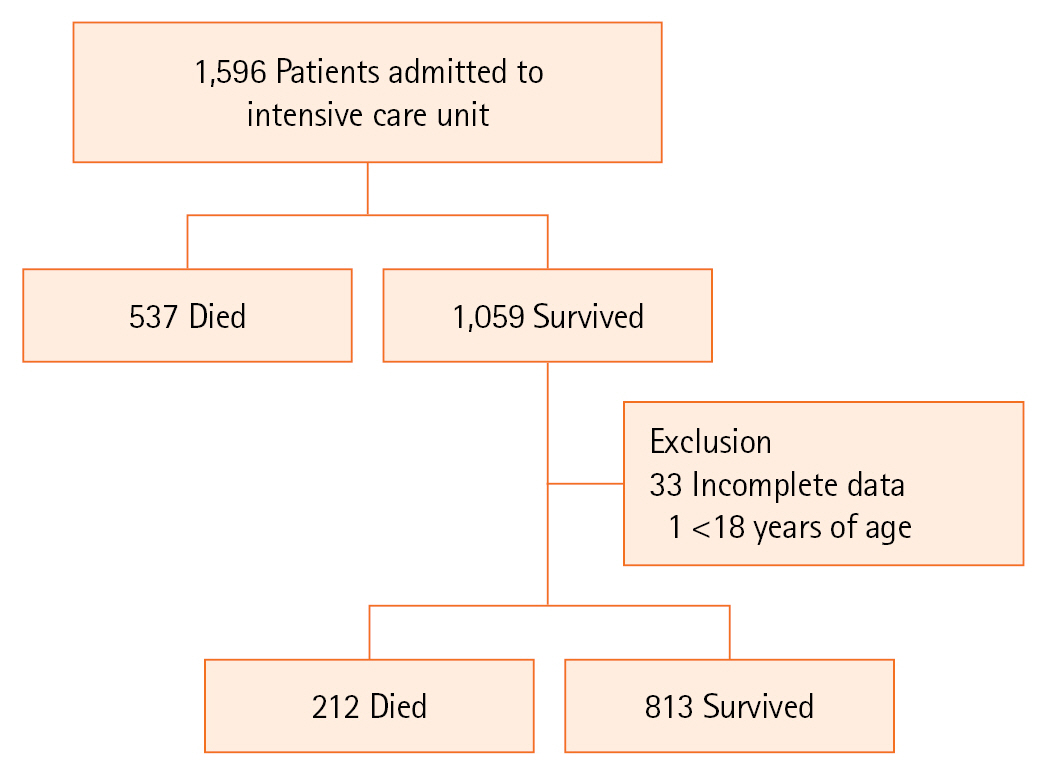
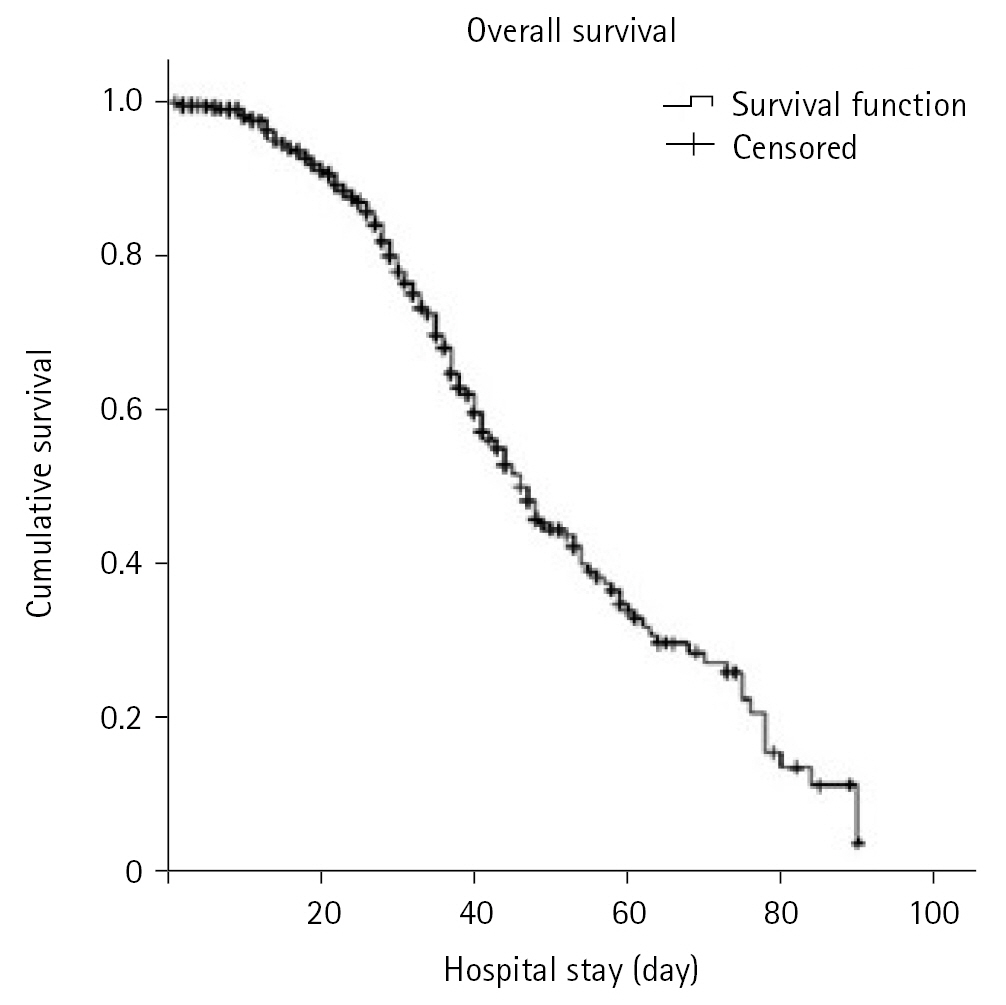
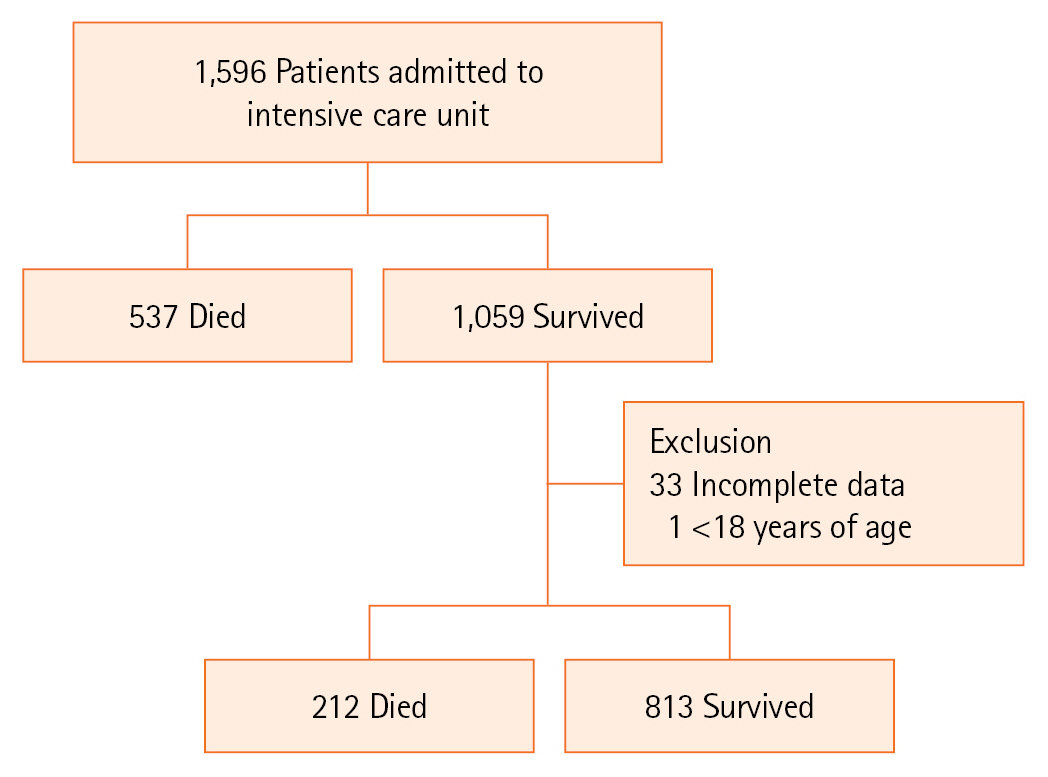
- A total of 1,025 patients who survived hospitalization in the ICU were analyzed, of which 212 (20.7%) died after leaving the ICU. When separating the groups of survivors and non-survivors according to hospital outcome, the median age was higher among non-survivors. Longer hospital stays and higher SAPS III values were observed among non-survivors. In the logistic regression, the variables age, length of hospital stay, SAPS III, presence of infection, and readmission to the ICU were associated with hospital mortality.
-
Conclusions
- Infection on ICU discharge, ICU readmission, age, length of hospital stay, and SAPS III score increased risk of death in ICU survivors.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
DISCUSSION
KEY MESSAGES
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
FUNDING
None.
-
AUTHOR CONTRIBUTIONS
Conceptualization: LGAS, ELL, CMCG. Data curation: LGAS, CMDMC, TBT, CMCG. Formal analysis: ELL. Methodology: LGAS, CMDMC, TBT, LTQC, CMCG. Project administration: CMCG. Visualization: all authors. Writing–original draft: LGAS, TBT. Writing–review & editing: CMC, LTQC, ELL, CMCG.
NOTES
Acknowledgments
| Variable | Survivor (n=813) | Non-survivor (n=212) | P-value |
|---|---|---|---|
| Age (yr) | 60 (44–72.5) | 67.5 (53–77) | <0.001a) |
| Male | 444 (54.6) | 129 (60.8) | 0.103b) |
| ICU length of stay (day) | 2 (1.5–6) | 9 (3–15) | <0.001a) |
| Hospital length of stay (day) | 14 (7–24) | 32 (20–45.7) | <0.001a) |
| SAPS III | 44 (34–58) | 61 (50.2–75) | <0.001a) |
| Reason for admission | <0.001b) | ||
| Clinical | 151 (18.5) | 80 (37.7) | |
| Elective PO | 394 (48.5) | 43 (20.3) | |
| Emergency PO | 138 (16.9) | 51 (24.1) | |
| Trauma | 130 (30.9) | 38 (17.9) | |
| BMI (kg/m2) | 25.7 (23.4–28.1) | 25.1 (23.0–27.9) | 0.524a) |
| Comorbidity | - | ||
| Hypertension | 346 (42.6) | 95 (44.8) | |
| Cancer | 65 (8.0) | 20 (9.4) | |
| Cirrhosis | 6 (0.7) | 4 (1.9) | |
| Congestive heart failure | 51 (6.3) | 19 (8.9) | |
| Coronary diseases | 38 (4.7) | 10 (4.7) | |
| COPD | 11 (1.3) | 8 (3.8) | |
| Diabetes mellitus | 139 (17.1) | 34 (16.0) | |
| Use of mechanical ventilation | 304 (37.4) | 141 (66.5) | <0.001b) |
| Infection | 197 (24.2) | 117 (55.2) | <0.001b) |
| Readmission to ICU | 25 (3.1) | 67 (31.6) | <0.001b) |
| Microorganism | - | ||
| Not identified | 73 (8.9) | 30 (14.2) | 0.026b) |
| Sensitive | 50 (6.1) | 28 (13.2) | 0.001b) |
| MDR | 29 (3.6) | 21 (9.9) | <0.001b) |
| XDR | 43 (5.3) | 38 (17.9) | <0.001b) |
| PDR | 2 (0.2) | 0 | 0.471b) |
| MDR/XDR/PDR | 74 (9.1) | 59 (27.8) | <0.001b) |
Values are presented as median (interquartile range) or number (%).
ICU: intensive care unit; SAPS: Simplified Acute Physiology Score; PO: postoperative; BMI: body mass index; COPD: chronic obstructive pulmonary disease; MDR: multidrug-resistant microorganisms (non-susceptibility to at least one agent in three or more antimicrobial categories); XDR: extensively drug-resistant (non-susceptibility to at least one agent in all but two or fewer antimicrobial categories); PDR: pandrug-resistant microorganisms (non-susceptibility to all agents in all antimicrobial categories).
a) Mann-Whitney test;
b) Chi-square test.
ICU: intensive care unit; CI: confidence interval; SAPS: Simplified Acute Physiology Score; MDR: multidrug-resistant microorganisms (non-susceptibility to at least one agent in three or more antimicrobial categories); XDR: extensively drug-resistant (non-susceptibility to at least one agent in all but two or fewer antimicrobial categories); PDR: pandrug-resistant microorganisms (non-susceptibility to all agents in all antimicrobial categories).
- 1. Goldhill DR, Sumner A. Outcome of intensive care patients in a group of British intensive care units. Crit Care Med 1998;26:1337-45.ArticlePubMed
- 2. Rowan KM, Kerr JH, Major E, McPherson K, Short A, Vessey MP. Intensive Care Society’s APACHE II study in Britain and Ireland--II: Outcome comparisons of intensive care units after adjustment for case mix by the American APACHE II method. BMJ 1993;307:977-81.ArticlePubMedPMC
- 3. Smith L, Orts CM, O’Neil I, Batchelor AM, Gascoigne AD, Baudouin SV. TISS and mortality after discharge from intensive care. Intensive Care Med 1999;25:1061-5.ArticlePubMedPDF
- 4. Azoulay E, Adrie C, De Lassence A, Pochard F, Moreau D, Thiery G, et al. Determinants of postintensive care unit mortality: a prospective multicenter study. Crit Care Med 2003;31:428-32.ArticlePubMed
- 5. Ranzani OT, Prada LF, Zampieri FG, Battaini LC, Pinaffi JV, Setogute YC, et al. Failure to reduce C-reactive protein levels more than 25% in the last 24 hours before intensive care unit discharge predicts higher in-hospital mortality: a cohort study. J Crit Care 2012;27:525. Article
- 6. Campbell AJ, Cook JA, Adey G, Cuthbertson BH. Predicting death and readmission after intensive care discharge. Br J Anaesth 2008;100:656-62.ArticlePubMed
- 7. Ponzoni CR, Corrêa TD, Filho RR, Serpa Neto A, Assunção MS, Pardini A, et al. Readmission to the intensive care unit: incidence, risk factors, resource use, and outcomes: a retrospective cohort study. Ann Am Thorac Soc 2017;14:1312-9.ArticlePubMed
- 8. Rodrigues CM, Pires EM, Feliciano JP, Vieira JM Jr, Taniguchi LU. Admission factors associated with intensive care unit readmission in critically ill oncohematological patients: a retrospective cohort study. Rev Bras Ter Intensiva 2016;28:33-9.ArticlePubMedPMC
- 9. Lin WT, Chen WL, Chao CM, Lai CC. The outcomes and prognostic factors of the patients with unplanned intensive care unit readmissions. Medicine (Baltimore) 2018;97:e11124.ArticlePubMedPMC
- 10. Hosein FS, Roberts DJ, Turin TC, Zygun D, Ghali WA, Stelfox HT. A meta-analysis to derive literature-based benchmarks for readmission and hospital mortality after patient discharge from intensive care. Crit Care 2014;18:715. ArticlePubMedPMCPDF
- 11. Keegan MT, Soares M. What every intensivist should know about prognostic scoring systems and risk-adjusted mortality. Rev Bras Ter Intensiva 2016;28:264-9.ArticlePubMedPMC
- 12. Serpa Neto A, Assunção MS, Pardini A, Silva E. Feasibility of transitioning from APACHE II to SAPS III as prognostic model in a Brazilian general intensive care unit: a retrospective study. Sao Paulo Med J 2015;133:199-205.ArticlePubMed
- 13. Magiorakos AP, Srinivasan A, Carey RB, Carmeli Y, Falagas ME, Giske CG, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect 2012;18:268-81.ArticlePubMed
- 14. Morland M, Haagensen R, Dahl FA, Berdal JE. Epidemiology and prognoses in a medical intermediate care unit. Tidsskr Nor Laegeforen 2018;138.ArticlePMC
- 15. Capuzzo M, Volta C, Tassinati T, Moreno RP, Valentin A, Guidet B, et al. Hospital mortality of adults admitted to intensive care units in hospitals with and without intermediate care units: a multicentre European cohort study. Crit Care 2014;18:551. ArticlePubMedPMCPDF
- 16. Hosein FS, Bobrovitz N, Berthelot S, Zygun D, Ghali WA, Stelfox HT. A systematic review of tools for predicting severe adverse events following patient discharge from intensive care units. Crit Care 2013;17:R102. ArticlePubMedPMC
- 17. Haniffa R, Isaam I, De Silva AP, Dondorp AM, De Keizer NF. Performance of critical care prognostic scoring systems in low and middle-income countries: a systematic review. Crit Care 2018;22:18. ArticlePubMedPMCPDF
- 18. Fuchs PA, Czech IJ, Krzych ŁJ. The pros and cons of the prediction game: the never-ending debate of mortality in the intensive care unit. Int J Environ Res Public Health 2019;16:3394. ArticlePubMedPMC
- 19. Donnelly JP, Wang XQ, Iwashyna TJ, Prescott HC. Readmission and death after initial hospital discharge among patients with COVID-19 in a large multihospital system. JAMA 2021;325:304-6.ArticlePubMed
- 20. Madotto F, McNicholas B, Rezoagli E, Pham T, Laffey JG, Bellani G, et al. Death in hospital following ICU discharge: insights from the LUNG SAFE study. Crit Care 2021;25:144. ArticlePubMedPMC
- 21. Santamaria JD, Duke GJ, Pilcher DV, Cooper DJ, Moran J, Bellomo R, et al. The timing of discharge from the intensive care unit and subsequent mortality: a prospective, multicenter study. Am J Respir Crit Care Med 2015;191:1033-9.ArticlePubMed
- 22. Azoulay E, Alberti C, Legendre I, Buisson CB, Le Gall JR, European Sepsis Group. Post-ICU mortality in critically ill infected patients: an international study. Intensive Care Med 2005;31:56-63.ArticlePubMedPDF
- 23. Barrasa-Villar JI, Aibar-Remón C, Prieto-Andrés P, Mareca-Doñate R, Moliner-Lahoz J. Impact on morbidity, mortality, and length of stay of hospital-acquired infections by resistant microorganisms. Clin Infect Dis 2017;65:644-52.ArticlePubMed
- 24. Serra-Burriel M, Keys M, Campillo-Artero C, Agodi A, Barchitta M, Gikas A, et al. Impact of multi-drug resistant bacteria on economic and clinical outcomes of healthcare-associated infections in adults: systematic review and meta-analysis. PLoS One 2020;15:e0227139.ArticlePubMedPMC
- 25. Rosa RG, Falavigna M, Robinson CC, Sanchez EC, Kochhann R, Schneider D, et al. Early and late mortality following discharge from the ICU: a multicenter prospective cohort study. Crit Care Med 2020;48:64-72.ArticlePubMed
- 26. Taniguchi LU, Ramos FJ, Momma AK, Martins Filho AP, Bartocci JJ, Lopes MF, et al. Subjective score and outcomes after discharge from the intensive care unit: a prospective observational study. J Int Med Res 2019;47:4183-93.ArticlePubMedPMCPDF
- 27. Kołpa M, Wałaszek M, Gniadek A, Wolak Z, Dobroś W. Incidence, microbiological profile and risk factors of healthcare-associated infections in intensive care units: a 10 year observation in a provincial hospital in Southern Poland. Int J Environ Res Public Health 2018;15:112. ArticlePubMedPMC
- 28. Ferreira LL, Azevedo LM, Salvador PT, Morais SH, Paiva RM, Santos VE. Nursing care in healthcare-associated infections: a scoping review. Rev Bras Enferm 2019;72:476-83.ArticlePubMed
- 29. Mota EC, Oliveira SP, Silveira BR, Silva PL, Oliveira AC. Incidência da pneumonia associada à ventilação mecânica em unidade de terapia intensiva. Medicina (Ribeirão Preto) 2017;50:39-46.ArticlePDF
- 30. Navon-Venezia S, Kondratyeva K, Carattoli A. Klebsiella pneumoniae: a major worldwide source and shuttle for antibiotic resistance. FEMS Microbiol Rev 2017;41:252-75.ArticlePubMed
- 31. de Maio Carrilho CM, de Oliveira LM, Gaudereto J, Perozin JS, Urbano MR, Camargo CH, et al. A prospective study of treatment of carbapenem-resistant Enterobacteriaceae infections and risk factors associated with outcome. BMC Infect Dis 2016;16:629. PubMedPMC
- 32. Breijyeh Z, Jubeh B, Karaman R. Resistance of Gram-negative bacteria to current antibacterial agents and approaches to resolve it. Molecules 2020;25:1340. ArticlePubMedPMC
- 33. Tejerina Álvarez EE, Gómez Mediavilla KA, Rodríguez Solís C, Valero González N, Lorente Balanza JÁ. Risk factors for readmission to ICU and analysis of intra-hospital mortality. Med Clin (Barc) 2022;158:58-64.ArticlePubMed
- 34. Londoño Restrepo J, Macias Ospina IC, Ochoa Jaramillo FL. Factores de riesgo asociados a infecciones por bacterias multirresistentes derivadas de la atención en salud en una institución hospitalaria de la ciudad de Medellín 2011-2014. Infect 2016;20:77-83.Article
- 35. Bergamasco E Paula R, Tanita MT, Festti J, Queiroz Cardoso LT, Carvalho Grion CM. Analysis of readmission rates to the intensive care unit after implementation of a rapid response team in a University Hospital. Med Intensiva 2017;41:411-7.ArticlePubMed
- 36. Jung B, Daurat A, De Jong A, Chanques G, Mahul M, Monnin M, et al. Rapid response team and hospital mortality in hospitalized patients. Intensive Care Med 2016;42:494-504.ArticlePubMedPDF
References
Figure & Data
References
Citations
- Analysis of the infectious agent’s structure and antibiotic resistance parameters in patients in intensive care units of a multidisciplinary hospital
O. I. Butranova, S. K. Zyryanov, A. A. Gorbacheva, G A. Putsman
Kachestvennaya Klinicheskaya Praktika = Good Clinical Practice.2024; (4): 4. CrossRef - Interpretability-based machine learning for predicting the risk of death from pulmonary inflammation in Chinese intensive care unit patients
Yihai Zhai, Danxiu Lan, Siying Lv, Liqin Mo
Frontiers in Medicine.2024;[Epub] CrossRef
 PubReader
PubReader Cite
Cite- Figure
-

- Related articles
-
- Risk factors for mortality in intensive care unit patients with Stenotrophomonas maltophilia pneumonia in South Korea
- Factors influencing sleep quality in the intensive care unit: a descriptive pilot study in Korea
- Reply to comment on “Risk factors for intensive care unit readmission after lung transplantation: a retrospective cohort study”
- Comment on “Risk factors for intensive care unit readmission after lung transplantation: a retrospective cohort study”
- Nosocomial meningitis in intensive care: a 10-year retrospective study and literature review

