Articles
- Page Path
- HOME > Acute Crit Care > Volume 39(1); 2024 > Article
-
Review Article
Meta-analysis The impact of ketamine on outcomes in critically ill patients: a systematic review with meta-analysis and trial sequential analysis of randomized controlled trials -
Yerkin Abdildin1
 , Karina Tapinova2, Assel Nemerenova1, Dmitriy Viderman3,4
, Karina Tapinova2, Assel Nemerenova1, Dmitriy Viderman3,4 -
Acute and Critical Care 2024;39(1):34-46.
DOI: https://doi.org/10.4266/acc.2023.00829
Published online: February 28, 2024
1Department of Mechanical and Aerospace Engineering, School of Engineering and Digital Sciences, Nazarbayev University, Astana, Kazakhstan
2Department of Emergency Medicine, Medical University of Vienna, Vienna, Austria
3Department of Surgery, School of Medicine, Nazarbayev University, Astana, Kazakhstan
4Department of Anesthesiology, Intensive Care, and Pain Medicine, National Research Oncology Center, Astana, Kazakhstan
- Corresponding author: Dmitriy Viderman Department of Surgery, School of Medicine, Nazarbayev University, 5/1 Kerey and Zhanibek Khandar St, Astana 020000, Kazakhstan Tel: +7-70-5542-6716, E-mail: dmitriy.viderman@nu.edu.kz
© 2024 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background
- This meta-analysis aims to evaluate the effects of ketamine in critically ill intensive care unit (ICU) patients.
-
Methods
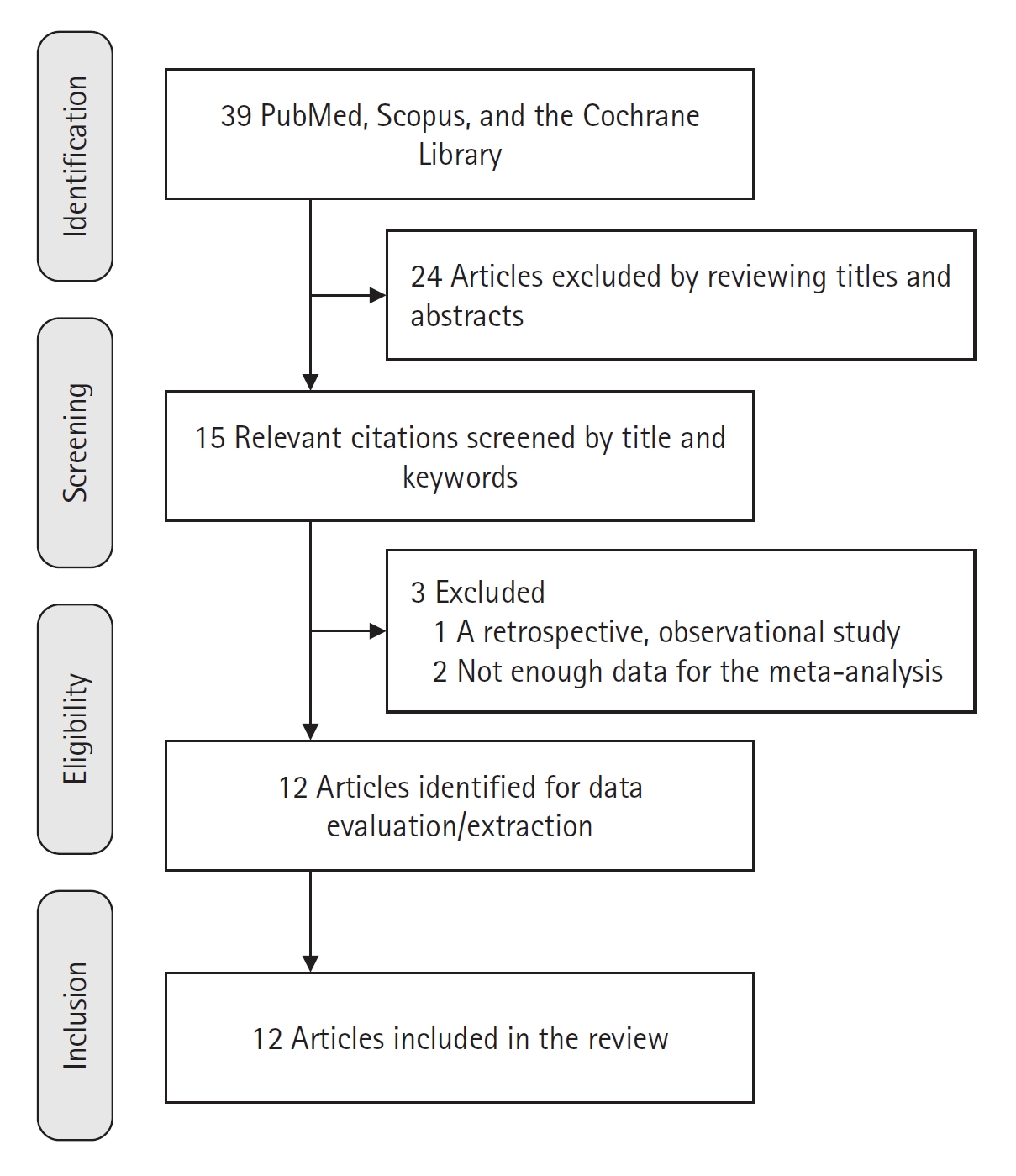
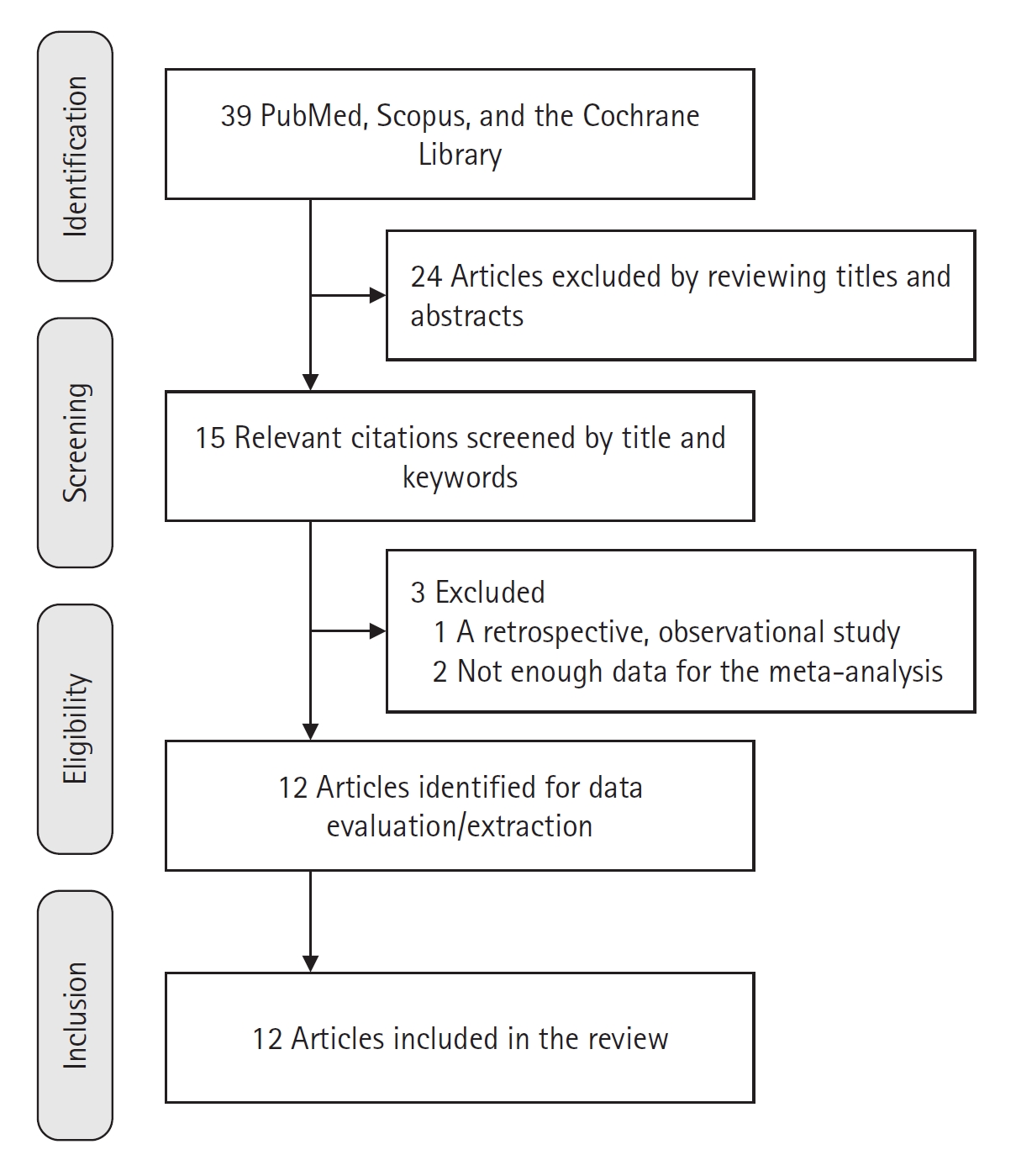
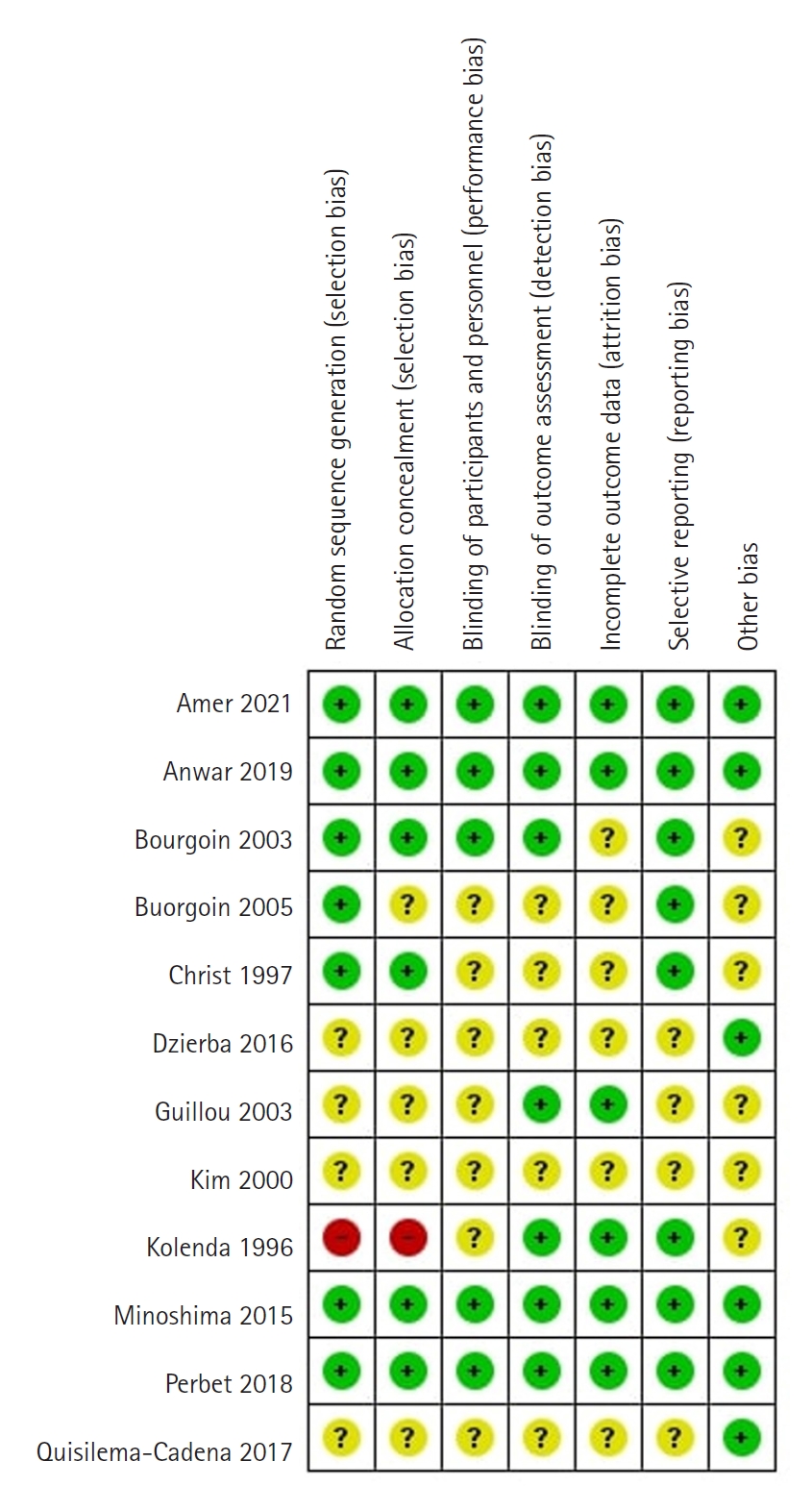
- The search for randomized controlled trials (RCTs) in PubMed, Scopus, and the Cochrane Library was performed initially in January but was repeated in December 2023. Included studies compared ketamine with other traditional agents used in the ICU. We synthesized evidence using RevMan v5.4, presenting the results as forest plots, and used trial sequential analysis (TSA) software v. 0.9.5.10 Beta, presenting results as TSA plots. Our outcomes were mortality, pain, opioid and midazolam requirements, delirium rates, and ICU length of stay.
-
Results
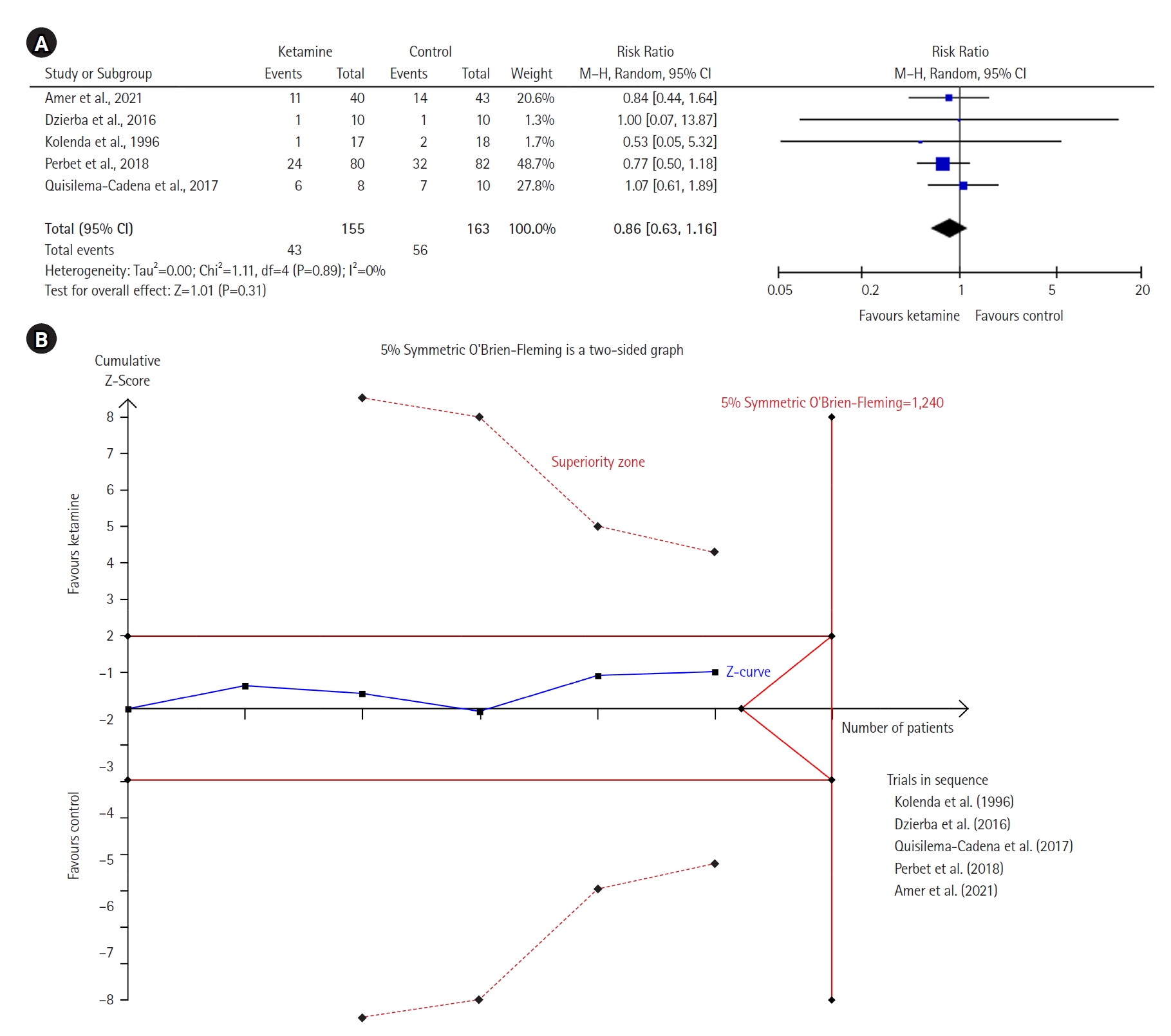
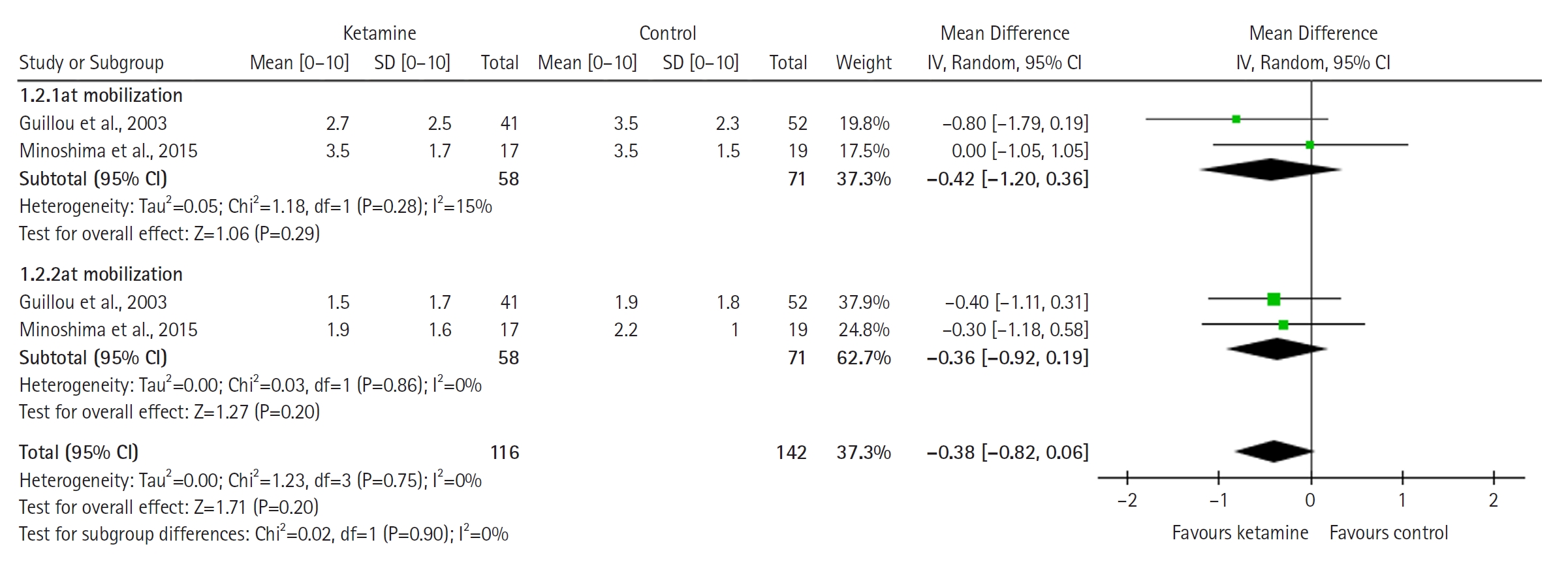
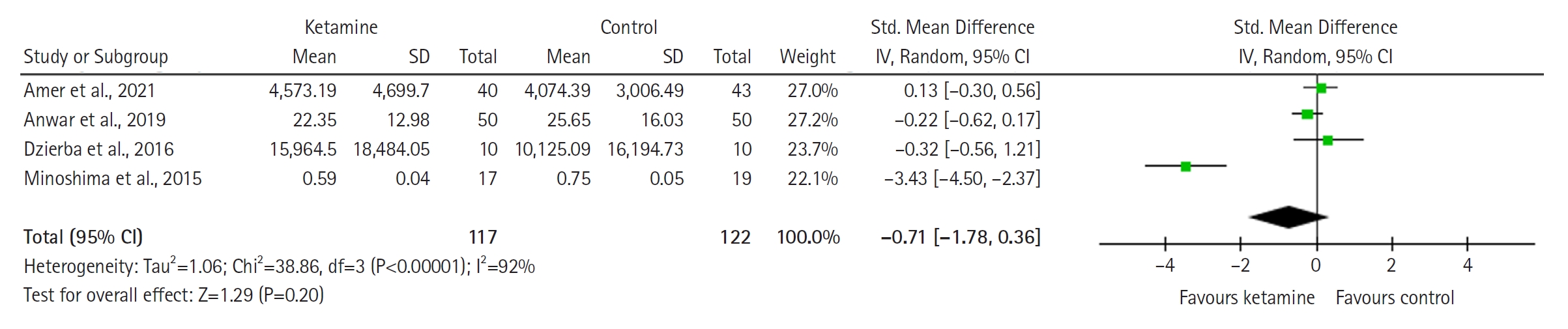
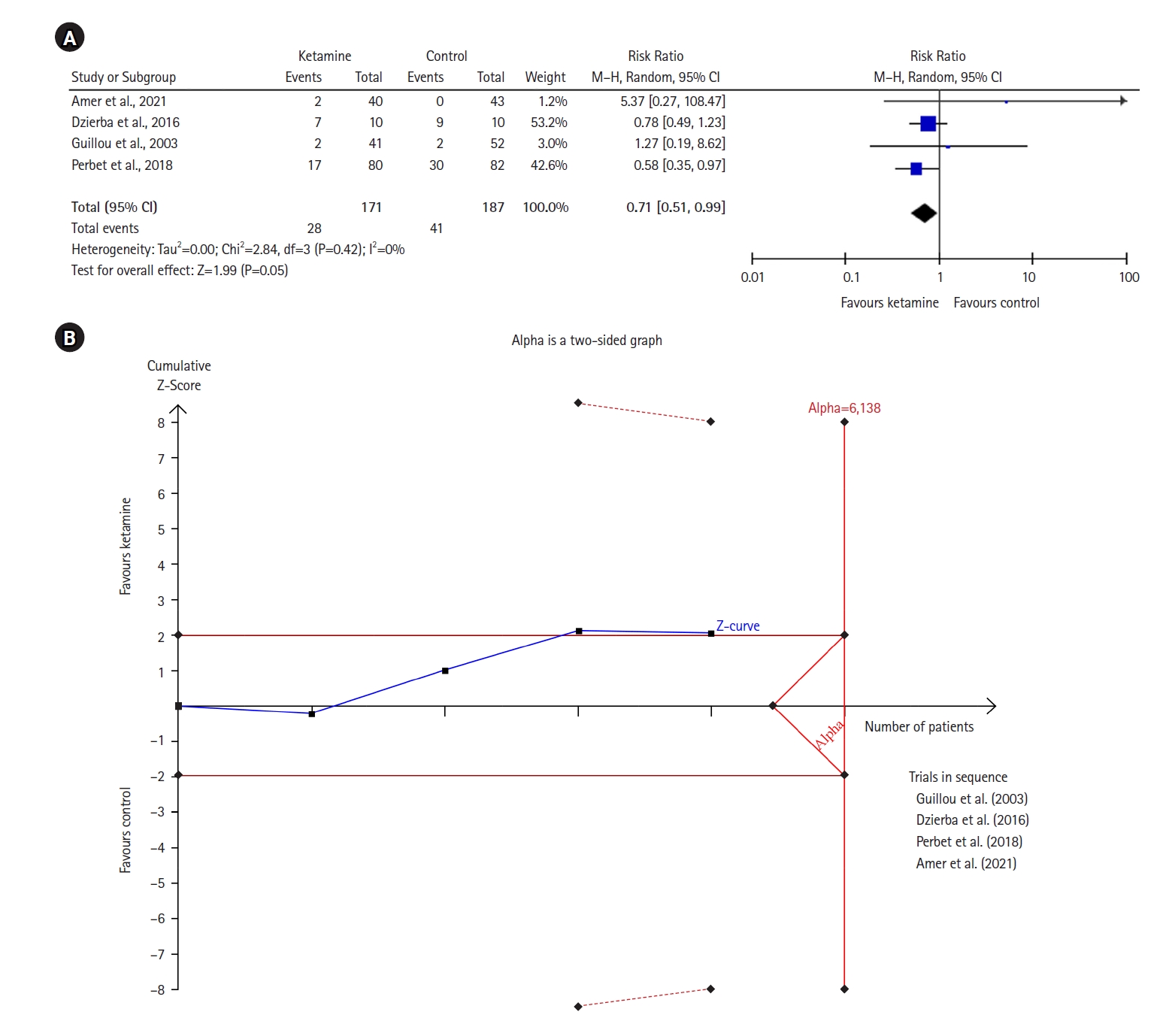
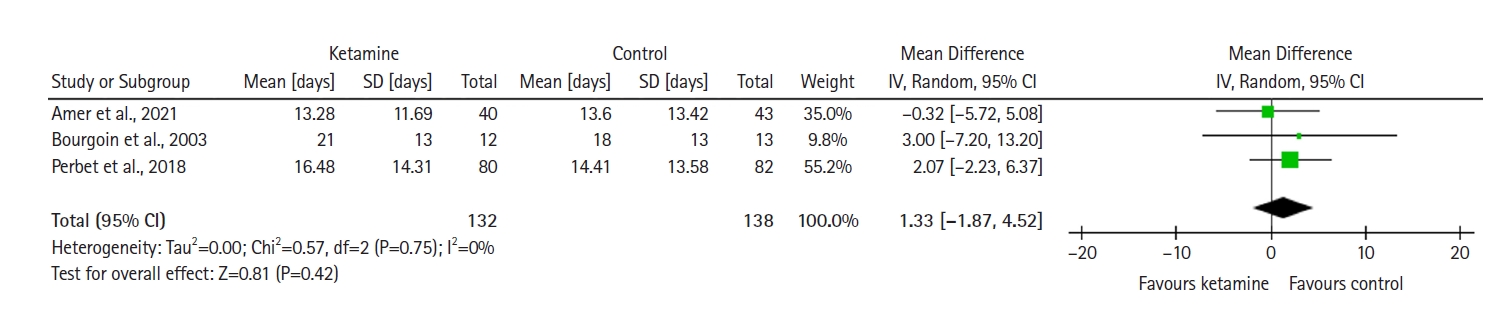
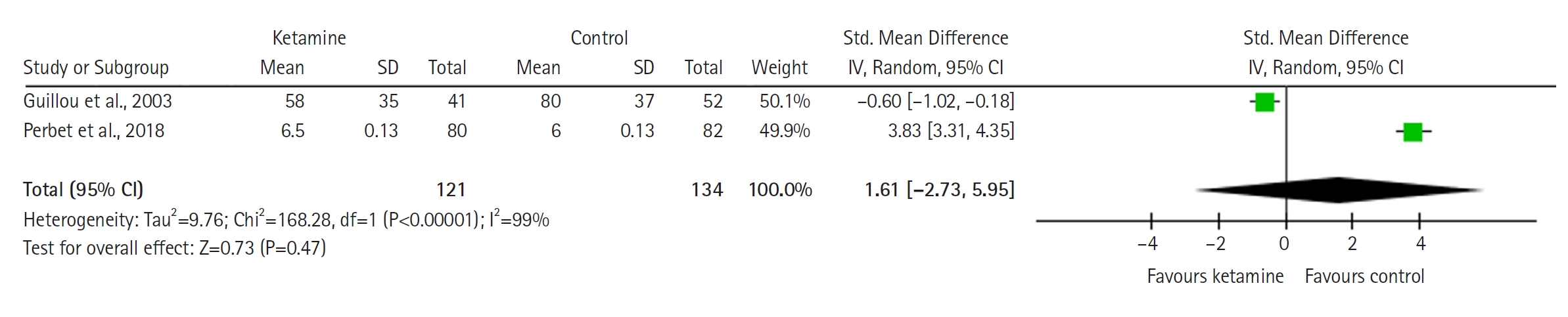
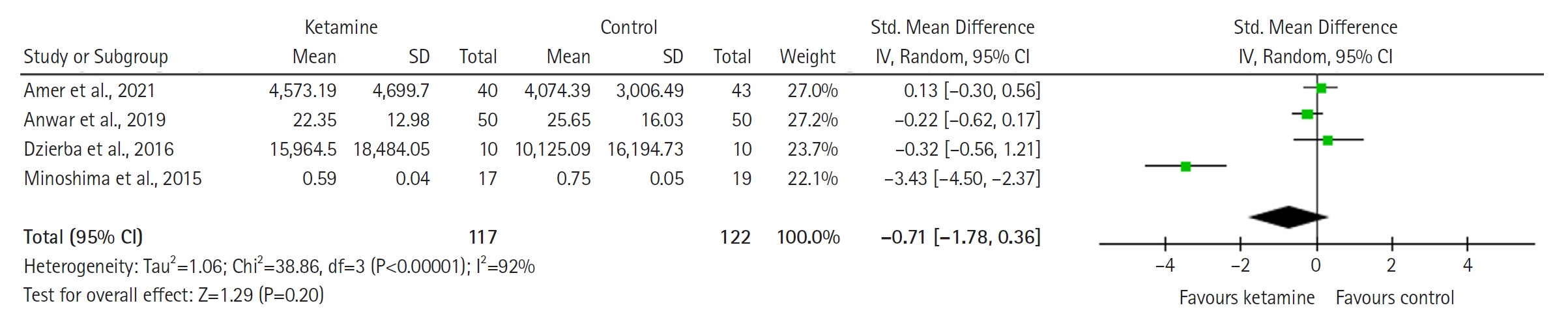
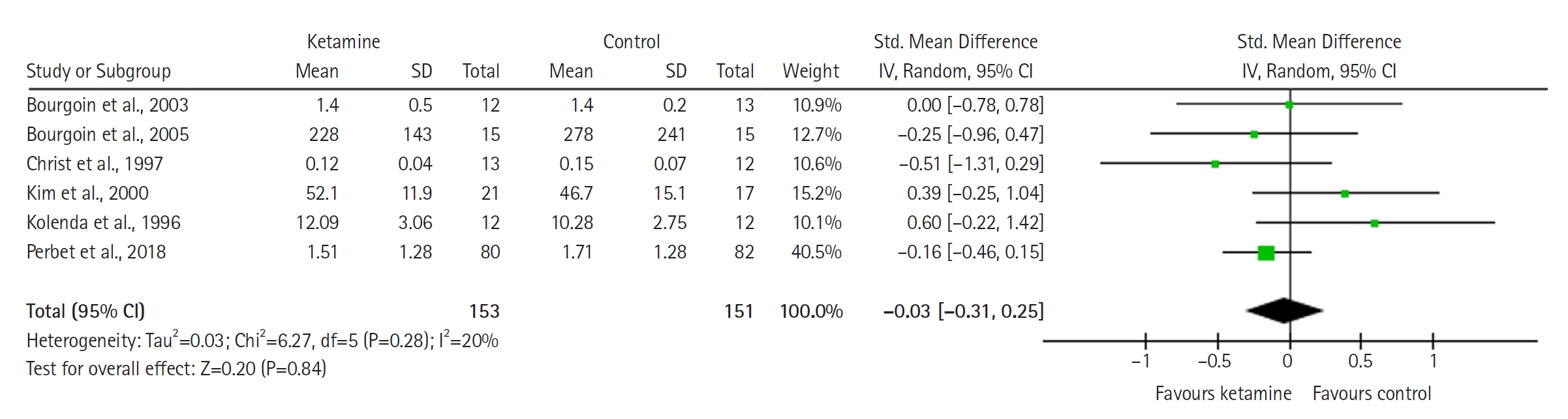
- Twelve RCTs involving 805 ICU patients (ketamine group, 398; control group, 407) were included in the meta-analysis. The ketamine group was not superior to the control group in terms of mortality, pain, mean and cumulative opioid consumption, midazolam consumption, and ICU length of stay. However, the model favored the ketamine group over the control group in delirium rate. This result is significant in terms of conventional boundaries (alpha=5%) but is not robust in TSA. The applicability of the findings is limited by the small number of patients pooled for each outcome.
-
Conclusions
- No differences were found between ketamine and control groups regarding any outcome except delirium rate, where the model favored the ketamine group over the control group. However, this result is not robust as sensitivity analysis and trial sequential analysis suggest that more RCTs should be conducted in the future.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
DISCUSSION
HIGHLIGHTS
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
FUNDING
This meta-analysis was supported by the Nazarbayev University Faculty Development Competitive Research (grants no. 11022021FD2906 and SOM2024005).
-
ACKNOWLEDGMENTS
None.
-
AUTHOR CONTRIBUTIONS
Conceptualization: DV. Methodology: YA, DV, KT. Supervision: DV. Funding: YA, DV. Validation: YA, DV. Data curation: AN, YA. Writing–original draft: all authors. Writing–review & editing: all authors.
NOTES




| Study | Country | Study design | Study goal | Type of ICU patients (brain injury, stroke, cardiac surgery, general ICU patients) | Primary diagnosis | Type of surgery | Age in the groups (yr) | Number of patients (intervention/control) | Groups (control; comparators) and specification | Dose of ketamine and duration of its infusion | Was mechanical ventilation used? | Study conclusion |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Amer et al. (2021) [40] | Kingdom of Saudi Arabia | RCT | Primary: median duration of MV, and ventilator-free days up to day 28 | Critically ill patients with MV | From text: ARDS (55%), solid organ transplantation/malignancy (25%), HIPEC, COVID-19 pneumonia, and sickle cell disease. | Postoperative abdominal surgery | Median (IQR): ketamine, 59 (40.5–73); | Intervention (ketamine): 40; control: 43 | Ketamine vs. control | Continuous adjunct ketamine infusion 1–2 μg/kg/min for 48 hours | Yes | Ketamine did not affect hemodynamics or other outcomes and was safe. |
| Secondary: ICU and hospital LOS, mortality rate, and percentage of AEs | Or From table: ARDS, sepsis or septic shock, cardiovascular, gastrointestinal, neurological, trauma | control, 61 (47.5–70) | ||||||||||
| Anwar et al. (2019) [41] | United Kingdom | RCT | Primary: the proportion of patients with clinically meaningful pain at 3 and 6 months after cardiac surgery | Patients that were scheduled to undergo cardiac surgery via sternotomy | Persistent pain | Cardiac surgery, breast surgery | Median (IQR): usual care, 68 (52–72); pregabalin alone, 68 (59–73); pregabalin and ketamine, 64 (54–72) | Usual care (control group): 50; pregabalin alone: 50; pregabalin and ketamine: 50 | Usual care vs. pregabalin vs. pregabalin+ketamine | 150-mg pregabalin capsules, alongside 48 postoperative hours of continuous ketamine infusion at 0.1 mg/kg/hr | Yes | Pregabalin helps to reduce postoperative pain after cardiac surgery if it is administered before surgery and given twice a day for 2 weeks after surgery. |
| Secondary: acute pain scores at the sternotomy and saphenectomy sites (numeric rating scale of more than 3, after three maximal coughs and dorsiflexion, respectively) alongside total morphine consumption, both measured at 24 hours after surgery. | ||||||||||||
| Bourgoin et al. (2003) [51] | France | RCT | Change in ICP and cerebral perfusion pressure, "mortality rate and neurologic outcome," "sedation cost" | Patients who have severe head injury | Head injury | Not specified | Mean±SD: ketamine, 30±11; sufentanil, 27±7 | Intervention (ketamine+midozolam),12; control (sufentanil+midozolam),13 | Ketamine vs. sufentanil (control) | The average continuous infusion rates on the 4 first days were 82±25 µg/kg/min ketamine and 1.6 ±0.5 µg/kg/min midazolam | Yes | It is possible to use ketamine-midazolam to maintain intracranial and cerebral perfusion pressures of patients with traumatic brain injury under MV. |
| Bourgoin et al. (2005) [52] | France | RCT | The effects of an increase in plasma concentrations of sufentanil or ketamine administered by target-controlled infusion on cerebral hemodynamics | Patients with severe traumatic brain injury | Brain injury (From the table) | Before protocol: 2 patients in each group underwent neurosurgery, 3 patients underwent other surgery (abdominal, orthopedics) in each group | Mean±SD: sufentanil, 29±12; ketamine, 29±11 | Sufentanil, 15; ketamine, 15 | Ketamine vs. sufentanil (comparators) | Continuous infusion of 1.0 µg/ml ketamine and 100 ng/mL midazolam; predictive plasma concentrations were adjusted step by step 0.5 µg/ml for ketamine and 50 ng/ml for midazolam. | Yes | Use of ketamine or sufentanil does not negatively affect cerebral hemodynamics of patients with head injury. |
| Christ et al. (1997) [43] | Austria | RCT | Comparison of the cardiovascular effects and catecholamine requirements of ketamine versus sufentanil infusions | Critically ill patients with catecholamine-dependent heart failure | Heart surgery | Mean±SD: ketamine, 61±14; sufentanil, 64±11 | Sufentanil, 12; ketamine, 13 | Ketamine vs. sufentanil (control) | Continuous infusion of 2.5±0.9 mg/kg/hr throughout the first 24 hours | Yes | Ketamine cannot be used for a long-termed sedation due to its negative cardiovascular effect. | |
| Coronary heart disease, anterior myocardial infarction, inferior myocardial infarction, cardiomyopathy, valvular heart disease, aortic stenosis, aortic stenosis and mitral regurgitation, myocarditis, heart surgery, coronary artery bypass graft, composite graft, mitral valve replacement, hemolytic uremic syndrome | ||||||||||||
| Dzierba et al. (2016) [50] | United States | RCT | Testing of the effect of continuous, low-dose ketamine infusion on opioid and sedative requirements | Patients requiring extracorporeal membrane oxygenation | Not specified | Not specified | Median (IQR): protocol group, 43 (36–52); control group, 44 (25–58) | Ketamine, 10; standard sedation, 10 | Ketamine+standard sedation (protocol) vs. standard sedation alone (control) | Ketamine was dosed as a 40 mg IV bolus followed by a continuous infusion at 5 micrograms/kg/min in addition to standard sedation practices. Ketamine was continued until the medical team chose to achieve wakefulness or for 7 days, whichever came first. | Yes | Mixture of standard sedation and ketamine does not result in lower opioid and sedative requirements. |
| Guillou et al. (2003) [48] | France | RCT | Evaluating the effect of small-dose ketamine on the consumption of morphine and on adverse effects in patients | Abdominal surgical ICU | No information | Abdominal surgery, hepatectomy, esophageal surgery | Mean±SD: ketamine, 60±16; morphine, 60±15 | Ketamine, 41; placebo, 52 | Placebo vs. ketamine | Continuous infusion of 0.5 mg/kg followed by a perfusion of 2 µg/kg/ min during the first 24 hours and 1 µg/kg/min during the following 24 hours | Yes | Small doses of ketamine is the useful addition to morphine for pain treatment for patients after abdominal surgery. |
| Kim et al. (2000) [7] | Korea | RCT | Study potential advantage of ketamine in patients with MV | Patients with MV | No information | Not specified | Mean±SD: 62.6±11.7 | Ketamine, 21; morphine, 17 | Ketamine vs. morphine | 52.1±11.9 mg/day for 24 hours | Yes | Ketamine can be a substitution for the morphine for sedation purpose in patients with MV. |
| Kolenda et al. (1996) [45] | Germany | RCT | Testing the use of ketamine in patients after head injuries and in cases of increased ICP; evaluation of ketamine therapy in comparison with standard analgosedation | Head-injured patients | Diffuse injury II | Not specified | Median (min–max): ketamine, 38 (18–72); fentanyl, 29 (16–59) | Ketamine, 17; control, 18 | Ketamine+midozalam vs. fentanyl+midozalam | 65 mg/kg/day for a period of 3 to 14 days | Yes | The use of ketamine is more expensive than the use of fentanyl, but it can be used as an alternative anesthesia for ICU patients with severe cardiovascular, pulmonal or gastro-intestinal problems due to its positive effect on blood circulation and gastro-intestinal motility. |
| Diffuse injury III | ||||||||||||
| Evacuated mass lesion | ||||||||||||
| Minoshima et al. (2015) [49] | Japan | RCT | Examination of effect of low-dose ketamine on postoperative morphine requirement and morphine-related adverse effects as nausea and vomiting after scoliosis surgery Primary: cumulative morphine consumption in the initial 48 hours after surgery Secondary: postoperative pain score, sedation score, incidence of nausea and vomiting, and antiemetic consumption in the 48 hours after surgerytients undergoing posterior correction surgery | No information | Idiopathic scoliosis surgery | Mean±SD: placebo, 14±2; ketamine, 15±2 | Ketamine, 17; placebo, 19 | Ketamine vs. placebo (control) | Continuous infusion at 2 μg/kg/min until 48 hours | Yes | The use of ketamine reduces the need for morphine and antiemetics within 48 hours after surgery. | |
| Perbet et al. (2018) [23] | France | RCT | Evaluation of the effect of ketamine infusion on opiates consumption when added to standard care in ICU patients requiring sedation for mechanical ventilation Primary: daily consumption of remifentanil in both groups Secondary: the incidence of delirium, mortality rates, ICU LOS | General ICU patients | Sepsis | Non-cardiac surgery | Mean±SD: ketamine, 63±15; placebo, 61±14 | Ketamine, 80; placebo, 82 | Ketamine vs. placebo (control) | Continuous infusion at 0.2 mg/kg/hr | Yes | Ketamine reduces the need for delirium and its duration in patients. |
| Quisilema-Cadena et al. (2017) [46] | Cuba | Randomized observational research | Evaluation of the sedoanalgesic action of the combination midazolam-morphine and midazolam-ketamine in critically ventilated patients | Critically ill patients with MV | Sepsis | Not specified | Mean±SD: morphine, 57.0±21.37; ketamine, 61.13±12.48 | Morphine, 10; ketamine, 8 | Morphine vs. ketamine | Every 6 hours, the level of sedation was determined using the Richmond scale; a 0.3 mg/kg ketamine bolus was administered as an attack dose, in 50 mL syringes of 0.9% NaCl in 5 minutes, while the infusion dose was in the range of 0.05 to 0.4 mg/kg/hr. | Yes | Ketamine can be used as a sedation of critically ill patients with MV as it has the same effectiveness as morphine. |
ICU: intensive care unit; RCT: randomized controlled trial; MV: mechanical ventilation; LOS: length of stay; AE: adverse events; ARDS: acute respiratory distress syndrome; HIPEC: hyperthermic intraperitoneal chemotherapy; COVID-19: coronavirus disease 2019; IQR: interquartile range; SD: standard deviation; IV: intravenous; ICP: intracranial pressure.
- 1. Wheeler KE, Grilli R, Centofanti JE, Martin J, Gelinas C, Szumita PM, et al. Adjuvant analgesic use in the critically ill: a systematic review and meta-analysis. Crit Care Explor 2020;2:e0157. ArticlePubMedPMC
- 2. Brinck EC, Tiippana E, Heesen M, Bell RF, Straube S, Moore RA, et al. Perioperative intravenous ketamine for acute postoperative pain in adults. Cochrane Database Syst Rev 2018;12:CD012033. ArticlePubMedPMC
- 3. Chan K, Burry LD, Tse C, Wunsch H, De Castro C, Williamson DR. Impact of ketamine on analgosedative consumption in critically ill patients: a systematic review and meta-analysis. Ann Pharmacother 2022;56:1139-58.ArticlePubMedPMCPDF
- 4. Hurth KP, Jaworski A, Thomas KB, Kirsch WB, Rudoni MA, Wohlfarth KM. The reemergence of ketamine for treatment in critically ill adults. Crit Care Med 2020;48:899-911.ArticlePubMed
- 5. Wang H, Wang C, Wang Y, Tong H, Feng Y, Li M, et al. Sedative drugs used for mechanically ventilated patients in intensive care units: a systematic review and network meta-analysis. Curr Med Res Opin 2019;35:435-46.ArticlePubMed
- 6. Koo BN, Koh SO, Park SY, Shim JK, Chon SS. Continuous infusion of ketamine in mechanically ventilated patient in septic shock with status asthmaticus. Korean J Crit Care Med 2000;15:108-12.
- 7. Kim TH, Lim CM, Shim TS, Lee SD, Kim WS, Kim DS, et al. Comparison of the efficacy between ketamine and morphine on sedation and analgesia in patients with mechanical ventilation. Korean J Crit Care Med 2000;15:82-7.
- 8. Jabre P, Combes X, Lapostolle F, Dhaouadi M, Ricard-Hibon A, Vivien B, et al. Etomidate versus ketamine for rapid sequence intubation in acutely ill patients: a multicentre randomised controlled trial. Lancet 2009;374:293-300.ArticlePubMed
- 9. Hughes S. Towards evidence based emergency medicine: best BETs from the Manchester Royal Infirmary. BET 3: is ketamine a viable induction agent for the trauma patient with potential brain injury. Emerg Med J 2011;28:1076-7.ArticlePubMed
- 10. Knack SK, Prekker ME, Moore JC, Klein LR, Atkins AH, Miner JR, et al. The effect of ketamine versus etomidate for rapid sequence intubation on maximum sequential organ failure assessment score: a randomized clinical trial. J Emerg Med 2023;65:e371-82.ArticlePubMed
- 11. Holland D, Glober N, Christopher S, Zahn E, Lardaro T, O'Donnell D. Prehospital sedation with ketamine vs. midazolam: repeat sedation, intubation, and hospital outcomes. Am J Emerg Med 2020;38:1748-53.ArticlePubMed
- 12. Panzer O, Moitra V, Sladen RN. Pharmacology of sedative-analgesic agents: dexmedetomidine, remifentanil, ketamine, volatile anesthetics, and the role of peripheral Mu antagonists. Anesthesiol Clin 2011;29:587-605.Article
- 13. Buchheit JL, Yeh DD, Eikermann M, Lin H. Impact of low-dose ketamine on the usage of continuous opioid infusion for the treatment of pain in adult mechanically ventilated patients in surgical intensive care units. J Intensive Care Med 2019;34:646-51.ArticlePubMedPDF
- 14. Hudetz JA, Patterson KM, Iqbal Z, Gandhi SD, Byrne AJ, Hudetz AG, et al. Ketamine attenuates delirium after cardiac surgery with cardiopulmonary bypass. J Cardiothorac Vasc Anesth 2009;23:651-7.ArticlePubMed
- 15. Smischney NJ, Beach ML, Loftus RW, Dodds TM, Koff MD. Ketamine/propofol admixture (ketofol) is associated with improved hemodynamics as an induction agent: a randomized, controlled trial. J Trauma Acute Care Surg 2012;73:94-101.PubMed
- 16. Zeiler FA, Teitelbaum J, West M, Gillman LM. The ketamine effect on ICP in traumatic brain injury. Neurocrit Care 2014;21:163-73.ArticlePubMedPDF
- 17. Hudetz JA, Pagel PS. Neuroprotection by ketamine: a review of the experimental and clinical evidence. J Cardiothorac Vasc Anesth 2010;24:131-42.ArticlePubMed
- 18. Chang LC, Raty SR, Ortiz J, Bailard NS, Mathew SJ. The emerging use of ketamine for anesthesia and sedation in traumatic brain injuries. CNS Neurosci Ther 2013;19:390-5.ArticlePubMedPMC
- 19. Kumar A, Kohli A. Comeback of ketamine: resurfacing facts and dispelling myths. Korean J Anesthesiol 2021;74:103-14.ArticlePubMedPMCPDF
- 20. Von der Brelie C, Seifert M, Rot S, Tittel A, Sanft C, Meier U, et al. Sedation of patients with acute aneurysmal subarachnoid hemorrhage with ketamine is safe and might influence the occurrence of cerebral infarctions associated with delayed cerebral ischemia. World Neurosurg 2017;97:374-82.ArticlePubMed
- 21. Erstad BL, Patanwala AE. Ketamine for analgosedation in critically ill patients. J Crit Care 2016;35:145-9.ArticlePubMed
- 22. Manasco AT, Stephens RJ, Yaeger LH, Roberts BW, Fuller BM. Ketamine sedation in mechanically ventilated patients: a systematic review and meta-analysis. J Crit Care 2020;56:80-8.ArticlePubMed
- 23. Perbet S, Verdonk F, Godet T, Jabaudon M, Chartier C, Cayot S, et al. Low doses of ketamine reduce delirium but not opiate consumption in mechanically ventilated and sedated ICU patients: a randomised double-blind control trial. Anaesth Crit Care Pain Med 2018;37:589-95.ArticlePubMed
- 24. Hovaguimian F, Tschopp C, Beck-Schimmer B, Puhan M. Intraoperative ketamine administration to prevent delirium or postoperative cognitive dysfunction: a systematic review and meta-analysis. Acta Anaesthesiol Scand 2018;62:1182-93.ArticlePubMedPDF
- 25. Mion G. Ketamine infusions for sedation in ICU. Anaesth Crit Care Pain Med 2019;38:397-8.ArticlePubMed
- 26. Perbet S, Godet T, Constantin JM. Ketamine infusion for sedation in ICU, response to Dr Mion. Anaesth Crit Care Pain Med 2019;38:399. ArticlePubMed
- 27. Viderman D, Aubakirova M, Nabidollayeva F, Yegembayeva N, Bilotta F, Badenes R, et al. Effect of ketamine on postoperative neurocognitive disorders: a systematic review and meta-analysis. J Clin Med 2023;12:4314. ArticlePubMedPMC
- 28. Viderman D, Nabidollayeva F, Aubakirova M, Yessimova D, Badenes R, Abdildin Y. Postoperative delirium and cognitive dysfunction after general and regional anesthesia: a systematic review and meta-analysis. J Clin Med 2023;12:3549. ArticlePubMedPMC
- 29. PRISMA [Internet]. PRISMA; 2023 [cited 2023 Apr 1]. Available from: http://www.prisma-statement.org/PRISMAStatement/.
- 30. Thorlund K, Engstrøm J, Wetterslev J, Imberger G, Gluud C. Trial sequential analysis (TSA). Copenhagen Trial Unit; 2011.
- 31. Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res 2018;27:1785-805.ArticlePubMedPDF
- 32. Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol 2014;14:135. ArticlePubMedPMCPDF
- 33. Cochrane. RevMan [Internet]. Cochrane; 2023 [cited 2023 Apr 1]. Available from: https://training.cochrane.org/online-learning/core-software/revman.
- 34. Kang H. Trial sequential analysis: novel approach for meta-analysis. Anesth Pain Med (Seoul) 2021;16:138-50.ArticlePubMedPMCPDF
- 35. Sanfilippo F, La Via L, Tigano S, Morgana A, La Rosa V, Astuto M. Trial sequential analysis: the evaluation of the robustness of meta-analyses findings and the need for further research. EuroMediterranean Biomed J 2021;16:104-7.
- 36. Wetterslev J, Thorlund K, Brok J, Gluud C. Trial sequential analysis may establish when firm evidence is reached in cumulative meta-analysis. J Clin Epidemiol 2008;61:64-75.ArticlePubMed
- 37. De Cassai A, Pasin L, Boscolo A, Salvagno M, Navalesi P. Trial sequential analysis: plain and simple. Korean J Anesthesiol 2021;74:363-5.ArticlePubMedPMCPDF
- 38. Castellini G, Bruschettini M, Gianola S, Gluud C, Moja L. Assessing imprecision in Cochrane systematic reviews: a comparison of GRADE and Trial Sequential Analysis. Syst Rev 2018;7:110. ArticlePubMedPMCPDF
- 39. Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 2011;343:d5928. ArticlePubMedPMC
- 40. Amer M, Maghrabi K, Bawazeer M, Alshaikh K, Shaban M, Rizwan M, et al. Adjunctive ketamine for sedation in critically ill mechanically ventilated patients: an active-controlled, pilot, feasibility clinical trial. J Intensive Care 2021;9:54. ArticlePubMedPMCPDF
- 41. Anwar S, Cooper J, Rahman J, Sharma C, Langford R. Prolonged perioperative use of pregabalin and ketamine to prevent persistent pain after cardiac surgery. Anesthesiology 2019;131:119-31.ArticlePubMedPDF
- 42. Bawazeer M, Amer M, Maghrabi K, Alshaikh K, Amin R, Rizwan M, et al. Adjunct low-dose ketamine infusion vs standard of care in mechanically ventilated critically ill patients at a Tertiary Saudi Hospital (ATTAINMENT Trial): study protocol for a randomized, prospective, pilot, feasibility trial. Trials 2020;21:288. ArticlePubMedPMCPDF
- 43. Christ G, Mundigler G, Merhaut C, Zehetgruber M, Kratochwill C, Heinz G, et al. Adverse cardiovascular effects of ketamine infusion in patients with catecholamine-dependent heart failure. Anaesth Intensive Care 1997;25:255-9.ArticlePubMedPDF
- 44. Garner O, Patterson J, Mejia JM, Anand V, Deleija J, Nemeh C, et al. Impact of ketamine as an adjunct sedative in acute respiratory distress syndrome due to COVID-19 Pneumonia. Respir Med 2021;189:106667. ArticlePubMedPMC
- 45. Kolenda H, Gremmelt A, Rading S, Braun U, Markakis E. Ketamine for analgosedative therapy in intensive care treatment of head-injured patients. Acta Neurochir (Wien) 1996;138:1193-9.ArticlePubMedPDF
- 46. Quisilema-Cadena JM, Cordero-Escobar I, González-Hernández O. Comparación de dos esquemas de sedoanalgesia: Hermanos Ameijeiras. Revista Mexicana Anestesiología 2017;40:155-61.
- 47. Schmittner MD, Vajkoczy SL, Horn P, Bertsch T, Quintel M, Vajkoczy P, et al. Effects of fentanyl and S(+)-ketamine on cerebral hemodynamics, gastrointestinal motility, and need of vasopressors in patients with intracranial pathologies: a pilot study. J Neurosurg Anesthesiol 2007;19:257-62.PubMed
- 48. Guillou N, Tanguy M, Seguin P, Branger B, Campion JP, Mallédant Y. The effects of small-dose ketamine on morphine consumption in surgical intensive care unit patients after major abdominal surgery. Anesth Analg 2003;97:843-7.ArticlePubMed
- 49. Minoshima R, Kosugi S, Nishimura D, Ihara N, Seki H, Yamada T, et al. Intra- and postoperative low-dose ketamine for adolescent idiopathic scoliosis surgery: a randomized controlled trial. Acta Anaesthesiol Scand 2015;59:1260-8.ArticlePubMed
- 50. Dzierba AL, Brodie D, Bacchetta M, Muir J, Wasson L, Colabraro M, et al. Ketamine use in sedation management in patients receiving extracorporeal membrane oxygenation. Intensive Care Med 2016;42:1822-3.ArticlePubMedPDF
- 51. Bourgoin A, Albanèse J, Wereszczynski N, Charbit M, Vialet R, Martin C. Safety of sedation with ketamine in severe head injury patients: comparison with sufentanil. Crit Care Med 2003;31:711-7.ArticlePubMed
- 52. Bourgoin A, Albanèse J, Léone M, Sampol-Manos E, Viviand X, Martin C. Effects of sufentanil or ketamine administered in target-controlled infusion on the cerebral hemodynamics of severely brain-injured patients. Crit Care Med 2005;33:1109-13.ArticlePubMed
References
Figure & Data
References
Citations
- Ketamine sedation in critically ill patients: Past, present and future
Sameer Sharif, Jay Prakash, Bram Rochwerg
Indian Journal of Anaesthesia.2024; 68(8): 674. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite